Here we go again, anti-vaxxers keeping on moving the goalpost to fit their belief instead to change to adjust it to the facts. First it was mercury, then it was formaldehyde, then aluminum, today the “ingredient du jour” is polysorbate 80 and tomorrow they will blame it to PBS saline solution.
The latest fad as I have seen is to blame polysorbate 80 as a source of “vaccine-injury” with the bold claim that it breaks down the blood-brain barrier (BBB). Lets put the fact straight and debunk this one for all. But what is even better is the “what if” counter-argument. What if polysorbate 80 was indeed a good ingredient? I will come to that later.
Polysorbate (aka Tween 80) is a amphiphile compound as you can see the molecular structure below (source Wikipedia):
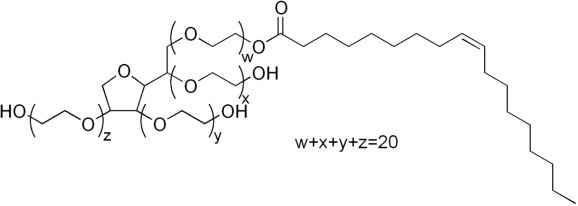
You can see the structure made of a lipophilic (loves fat) tail and a series of hydrophilic (loves water) tails, loaded with oxygen and hydroxyl groups. This is a typical structure of a detergent: one side will mix well with water, the other will mix very well with fat and oils. The result? You can form microspheres that can dissolve well in water and dissolve fat into water. This is how a detergent works, it helps to breakdown fats into small spheres and dissolve them in the drain water.
Polysorbate 80, due to this property, is very good to dissolve drugs and medicines that under normal condition would barely dissolve into biological fluids. This is why we have it in vaccines, but we also have it in medicines. Thats the job of biopharmaceutics: finding formulations to dissolve drugs into the body and allow them to reach a concentration high enough to display their therapeutic activity.
The use of polysorbate 80 in drug delivery of anti-cancerous drug is probably the first and foremost main driving factor on investigating its effect on the BBB. Brain tumors (primary and metastatic alike) are up until now one of the most dreaded and deadliest form of cancer. For instance, the average expected lifespan upon diagnosis of a grade IV glioma (aka glioblastoma multiforme) is grim: 18-months, with less than 5% survival after 5 years. The major issue is being able to deliver drugs and chemotherapy across the BBB. As reported by Pr. William Partridge (UCLA) the BBB remains the bottleneck in drug development for the treating neurological disorders (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC539316/?fref=gc&dti=873247819461536)
The first report of the investigation of polysorbate 80 on the BBB is probably by Spiegelman and colleagues in 1984 (http://thejns.org/doi/pdf/10.3171/jns.1984.61.4.0674), investigating the effect of the solvent used in etoposide solution for treating cancer. According to their result, they noted a statistical difference in the BBB permeability (using Evans Blue and 99mTc as tracers) following the injection of 1.125ml/kg. According to their paper, 5mL solution contained 400mg of polysorbate 80 or a concentration of 80mg/mL. Based on this, we can assume that the BBB effect was observed for a dose of 90mg/kg. Thats a very huge dose.
If we go back to the manure anti-vaxxers say, the amount injected via vaccines is enough to cause a barrier opening. According to John Hopkins University Institute of Vaccine Safety (http://www.vaccinesafety.edu/components-DTaP.htm), the expected concentration of polysorbate is lesser or equal to 100mcg or micrograms. Thats 0.1mg per dose. If we assume such dose is injected to a newborn (average weight ~3 kgs), then the amount injected is about 0.033mg/kg. Thats 2700 times less than what has been reported to induce a BBB disruption. Also you have to factor the bioavailability of polysorbate (that is 100% upon IV route) making this number a very optimistic number.
Now, the interesting twist about polsyorbate 80 is its use to enhance some drug carriers and its widely used for finding novel formulation to enhance the delivery of anti-cancerous drugs across the BBB. You can find a list of publications on Pubmed about that aspect (https://www.ncbi.nlm.nih.gov/pubmed/?term=polysorbate+80+blood-brain+barrier). What if polysorbate 80 not only will not injure your brain, but actually may help deliver drugs to help your brain fight disease?
Keep in mind that polysorbate 80 is good at dissolving lipid in water solutions but it is not good to let charged molecules accross the BBB, just in case someone comes with the claims that it conjugates with aluminum. Thats some high-school chemistry level.

24 replies on “[BBB/Junk Sciences] Polysorbate 80 and the BBB or how to put anti-vaxxers into a blowing cognitive dissonance”
“[Polysorbate-80 modified neurotoxin nanoparticle with its transport and cytotoxicity against blood-brain barrier].
[Article in Chinese]
Zhao YM1, Xia AX, Wei YH, Ruan YP, Li FZ.
Author information
Abstract
This study was aimed at the transport across blood-brain barrier (BBB) of polysorbate-80 modified neurotoxin loaded polybutylcyanoacrylate nanoparticle (P-80-NT-NP) and its cytotoxicity. An in vitro model of BBB using rat brain microvascular endothelial cells (rBMECs) was established. The cytotoxicity of P-80-NT-NP was measured by the MTT assays, where neurotoxin (NT), nanoparticle (NP), neurotoxin nanoparticle (NT-NP) as control, and the permeability of P-80-NT-NP was determined by using of Millicell insert coculture with rBMECs and fluorescence spectrophotometry. MTT results showed that NT, NP, NT-NP and P-80-NT-NP were avirulent to rBMECs when the concentration of NT was lower than 200 ng x mL(-1). But the cytotoxicity of NP, NT-NP and P-80-NT-NP would be augmented accordingly as concentration increased (P 0.05). When the concentration of NT was 150 ng x mL(-1), the permeability on rBMECs of P-80-NT-NP and NT-NP were both significantly higher than that of NT (P < 0.01), and the permeability of P-80-NT-NP was greater than that of NT-NP (P < 0.05). In conclusion, polysorbate-80 modified neurotoxin nanoparticles can transport across the BBB, while concentration of NT is greater than 200 ng x mL(-1), P-80-NT-NP has a little cytotoxicity against rBMECs.
https://www.ncbi.nlm.nih.gov/pubmed/21348312
LikeLike
The article is in Chinese, unless you can read Mandarin there is little we can discuss on it except that here PS80 was used as a delivery vector to enhance the delivery of a neurotoxin across the BBB. Unless you increased the dose of NT, no cytotoxic effect of PS80 combined with NT was observed.
That’s according to their English abstract.
LikeLike
“The BBB, like cell membranes in general, is subject to solvent-mediated disruption with chemicals such as ethanol, dimethylsulfoxide (DMSO), or detergents such as SDS, or Tween 80 also known as polysorbate-80.27–30 There are numerous examples in the literature where the peripheral administration of a drug, which normally should not cross the BBB, is followed by pharmacological activity in the brain. Such an observation could arise because the drug is transported across the BBB via an endogenous transport system. However, an alternative explanation is that the drug is injected in a diluent that is membrane destabilizing, and causes BBB disruption. Often the drug is solubilized in solvents such as ethanol or DMSO, or surfactants such as SDS, a Tween detergent, or other surfactants, such as polyethyleneglycol hydroxy stearate. Doses of solvents such as ethanol or DMSO at a level of 1-4 g/kg may cause solvent-mediated disruption of the BBB.27,28 This dose of DMSO or ethanol is given to animal models with surprising frequency, particularly small rodent models such as mice, which weigh only 20-30 g. The administration of just 50 μl of 50% DMSO to a 20-g mouse is equivalent to 1.25 g/kg DMSO, and there are examples in the literature of pharmacologic effects achieved in brain following systemic administration of drugs that normally do not cross the BBB. These drugs are administered in solvents such as ethanol or DMSO and the dose of solvent is such that BBB disruption may be caused by administration of the drug/solvent mixture. Tween 80, also known as polysorbate-80, is frequently administered in CNS drug formulations. A dose of polysorbate-80 of 3-30 mg/kg will cause BBB disruption in mice.30 Analgesia with kyotorphin, a oligopeptide that normally does not cross the BBB, is possible following the peripheral administration of the peptide, providing Tween 80 is coadministered.31 Low doses of another surfactant, SDS, are frequently included in CNS drug diluents. However, doses of SDS as low as 1.0 μg/kg can cause disruption of the BBB for short periods. Immune adjuvants such as Freund’s complete or incomplete adjuvant cause disruption of the BBB to circulating IgG that can persist for weeks.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC539316/
LikeLike
PS80 by its own is very unstable in vivo because of the esterases present in plasma that will chop it into pieces. Injection sites and dose matter.
Here a study that investigated the PK profile of PS80.
http://clincancerres.aacrjournals.org/content/5/10/2918
LikeLike
[…] Polysorbate 80 and the BBB or how to put anti-vaxxers into a blowing cognitive dissonance […]
LikeLiked by 2 people
[…] quick note on polysorbate 80 here because I don’t have the time to give a comprehensive chemistry […]
LikeLiked by 2 people
I really don’t understand how this article helps to debunk any myths. Polysorbate 80 may well be very helpful in delivering medication to the brain for treatment but for a parent trying to decide whether to vaccinate your article actually create some more questions. I went to the dr after my daughter suffered an injury with a clean piece of stainless steal. He wanted to give her a tetanus shot (it was actually a cocktail of 5 injections as they didn’t have just the tetanus). I asked to see the ingredient list and right next to aluminium was polysorbate 80. He couldn’t be tell me why that would be in there and didn’t even know what it did. I told him and he still couldn’t answer. I asked him what the effects of these heavy metals passing across the BBB would be and all he could honestly say was “well I’m not sure”.
I want truth and balanced arguments (based on true science)…. that’s what people need when deciding and this article was clearly skewed from the first sentence. From a place of frustration and condemnation rather than balance and truth.
LikeLiked by 1 person
Hi Rebekah,
Thank you for your comment. Lets discuss your comment into two steps:
1. PS80. PS80 is an emulsifier that helps dissolve hydrophobic (hates water) substances into aqueous substance. It helps create an interface between hydrophobic substances and water to mix together. This is why we use in ice-cream. Proteins are formed by amino acids, some of them are hydrophobic. These proteins fold as an origami and must maintain their native form to remain active for the immunization (by looking like the real protein found on bacteria and viruses surface). This folding is influenced by pH, temperature, salinity and others. PS80 help stabilize this origami and maintain it stable over time. Now to open the BBB with PS80, you need to inject 2700 doses straight into your veins to hope to see something to happen.
2. Aluminum. First, lets name it properly. It is a metalloid, very distinct atomic structure and chemical properties of heavy metals. Second, the amount crossing the BBB is minimal. Only 0.6% of plasma concentration will cross the BBB (via solute transporters). Al injected from vaccines do not reach the circulation at once with 100%. It is slowly released from the injection site and reach the bloodstream at a rate of 0.6% per day. It is like adding a teaspoon of Al into a 1lb bag of aluminum everyday while removing three tablespoons each day. Unless you have a severe kidney or you have an IV line feeding you or your child, there is no particular concern about Al in vaccines.
3. PS80 and Al. Some think that PS80 will help Al to cross the BBB. First, at the amount found in vaccines, you dont have enough to open the BBB. Second, if PS80 would help Al to cross the BBB, it would need to act as a chelator. This is where those making that claim failed their chemistry class in HS, in particular a course called “complexation chemistry”. It does not have the backbone needed to trap Al as a chelator.
Now that your concerns have been answered, do you still have concern about vaccines?
LikeLike
A recent 2018 study doi: 10.1016/j.cyto.2018.04.037.
“IL-4 mediates the delayed neurobehavioral impairments induced by neonatal hepatitis B vaccination that involves the down-regulation of the IL-4 receptor in the hippocampus” results showed:
3) peripheral IL-4 is able to penetrate into the hippocampus during the neonatal period; and
4) the permeability of the BBB in neonatal mice might explain the penetration of
peripheral IL-4 into the brain
Perhaps further work in a few years will explain the mechanisms of the permeability of the BBB in neonates.
LikeLiked by 1 person
Hi Nathan,
I guess this is the paper you are referring to?
https://www.sciencedirect.com/science/article/abs/pii/S104346661830190X
So here is the main problem with the experimental method of the author that have been plaguing them since 2016 (when they started this kind of study).
1. They consider a P0 mice pup equals to a newborn. The problem is it is not. Brain angiogenesis and subsequently BBB maturation in rodents at this stage is still in formation until P33 (https://www.sciencedirect.com/science/article/pii/S016538069900125X?via%3Dihub).
2) If we follow brain development, then the protocol should start at P7 at earliest:
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3737272/)
3) The authors injected the HBV vaccines via IP route. The IP route ~ to an IV injection in terms of PK profile. Since when are we injecting vaccines straight into a vascular route?
4) The timing between the different injections can be problematic, even more since we have a poor documentation of the HBV pharmacokinetics. How is 1 week interval matching the miminum of 4 and 8 weeks requested for the second and third injections?
Their studies are interesting but also have limitations that need to be accounted. One thing that bothers me is the authors claiming they validated their protocol in their 2016 paper and that it matches the human development. Yet, their 2016 papers showed nothing of that sort (they will send you to their supplementary figures but it is nowhere to be seen).
LikeLike
Thanks for replying.
I guess there are always improvements to be made with these studies.
Is there any way to contact them regarding chosen mice age or the supplementary tables? In the 2016 paper it does say “Although it is difficult to make the chosen ages of mice strictly correspond to those of humans, P0-P7-P21 was verified to be appropriate in a preliminary study (design: Table S1; results: Table S2 and Fig.S1)”
But the result in these three studies should at least indicate the need for precaution when administering the Hepatitis B vaccines especially for preterm infants.
IP route is recommended for animal experiments, it difficult to do it intramuscular. How else would you do it?
The timing is cosidered “appropriate” to correspond to those of humans according to the study. So again what would be more appropriate?
There are no studies of this sort on humans yet all newborns in the modern world are recommended to take this shot. It’s not like they can perform the exact same study on humans seeing what they need to do with the mice brains.
So I don’t see the need to be so alarmed at some new parents who prefer not to use this product for their hours old precious baby. Nowadays I regularly see the insane fear and smear campaign against the so called Anti Vax in the media and governement’s coercive legislations to “force” people to use the products without question when the informed choice really belong to the new parents.
LikeLiked by 1 person
In theory, yes you can contact the corresponding author about the data. But nothing force them to answer to you if they feel not.
Now in regards of preterms and HBV, your concern is valid and sound. This is I think where epidemiological studies are useful and needed so we can track how HBV impact the cognitive development of preterms. If you find any papers about this, feel free to share, would be more than happy to do so.
For the route, remember IP is almost IV route. So we are dealing with a global immune response. For vaccines, we are expecting a local immune response. If IM cannot be possible, then SC is an alternative route to keep it local (and fairly easy to do even on newborn pups, if you inject SC on the back).
If you follow this paper (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3737272/), then starting the HBV at P7 would be more relevant to humans, at least based on brain development standpoint. The paper was published in 2013 and this group has been investigating HBV since 2016.
The problem also we have is the PK profile of HB antigens, how long it takes to clear them out? The minimum time period in humans between two doses is 4 weeks. By that time, how much HBV vaccine particles are still detected? How much still remains in mice after 1 week? The answer right now is we dont really know much and I think this is an important missing point for this study. Is 1 week interval too short, too long or just right in terms of reflecting the immunization schedule.
LikeLike
“I really don’t understand…”
Yeah, no kidding.
Your story has a few holes:
– What tetanus shot exists as a cocktail of 5? You either have Td, TDaP, or DTaP. Only three different antigens present, at most. Where do you get 5?
– Aluminum is not listed as an ingredient because aluminum is not used. Elemental aluminum, which you AV zealots are so quick to clutch your pearls over, is not the same thing as an aluminum salt. Chemistry matters and I suggest you log off Facebook and take a basic chemistry course.
– Why would doctors know each and every ingredient that goes into a vaccine? They’re not making them. They’re not sourcing the materials to give to the pharmaceutical companies. Do you expect them to know every compound found in everything they use in their office? That’s asinine.
– And by all means I would LOVE for you to enthrall is with what PS80 does in a vaccine. No Googling and no going to your echo chamber for help!
LikeLiked by 2 people
The DTaP-HIB-IPV and DTaP-Hep B-IPV both contain 5 antigens.
LikeLiked by 1 person
Jackon’s point 3 about “Why would doctors know each and every ingredient that goes into a vaccine?”
Well like a waiter at a restaurant, if a customer asks what ingredients are in the food they should know at least the basics and if not then find out and let the customer know. If the customer shows concerns and the waiter is unsure then it’s best to find out more details before serving it.
This has to do with knowing what is going into your own body. Nothing to do with anti anything.
LikeLike
Hi Nathan, thank you for your comment.
I think comparing a doctor to a waiter is a bit condescending. I would compare it to a chef instead.
I would plays the devil’s advocate here. If the doctors job was solely administering vaccines, then yes he or she should know about every single bits of ingredients inside. However, those doctors who administer shots are either family medicine specialists (what we refer as GPs in UK) or pediatricians. You can imagine the vast and versatile amount of information they have to memorize is huge. Coupled with the selectivity of our memory (we trend to forget a lot of information we have learned, especially when we are conditioned to binge/purge for exams like it happens in med school), you trend to forget the information that is not requested on a daily basis. This is one of the different challenging factoring the difficulty to identify a rare disease right on the spot.
We also train HCW to know about the main active ingredient in medications (including vaccines) about the MOA, their adverse/side effects, their dosage, their contra-indications. We rarely spend time talking about the excipients (basically the rest of it) because they are considered inactive.
Asking a doctor to remember every single ingredient in vaccine is like asking a chef to give you the exact chemical composition (proteins, lipids, carbohydrates, compounds from plants secondary metabolism…) of each igredients used in their dish. The majority of this kind of information is mostly irrelevant for the final product (dish) but knowing the flavors and interactions between them (and the right dosage) matters more.
Now, you also have a valid point that the doctor should still have a basic knowledge of them and that would be something useful to have in their CE.
LikeLiked by 1 person
It wasn’t meant to be condescending at all.
Anyway if the doctor is compared to the chef then who is the manufacturer of products? Doctors don’t make the vaccines. Maybe in my previous scenario instead of serving “food”, the waiter should be serving bottled “drinks”. That might make more sense when comparing it to a doctor who are administering vaccines.
While I totally agree with the vast amount of information the doctors might need to memorise, it is these seemingly “inactive” expicients combined with adjuvants and other components that may have systemic effects on newborns and developing children. So for the bottled drinks in this new scenario I would ask the waiter if I could see the bottle with the list of ingredients to make sure whatever ingredients it may be, I can ask the waiter for more information and I get to decide whether to consume it. While some people might not be concerned about what they consume that is their business. And the same applies to products such as vaccines, if the cosumer has questions and after understanding all the information that has been provided and decides not to use it then that’s their choice.
No anti- required.
LikeLiked by 1 person
I completely agree with you that the consumer has the right to know the ingredients in a bottled drink. But should we reasonably expect the waiter to know the exact ingredients composition of 100 bottled drinks at any time and give an answer right away? He/she may remember the flavors of 100 bottled drinks, but asking him/her the exact composition of them at any time is in my opinion too much to ask. Remember, peds and GPs are not just giving shots, they are also taking care of other drugs. But I think here a cheat-sheet or a simple fact-sheet from the CDC that can be handled over to the parent maybe a better option.
LikeLiked by 1 person
Only problem here is we are not taking into account the full skull structure of an infant versus a fully developed adult…. Let me guess, off the top of the brain… a child’s brain isn’t fully encapsulated until a little after a year old…?
LikeLiked by 1 person
I am curious, how does a skull structure has to do with PS80? Brain angiogenesis is done, neuronal migration in their respective cortical layers is done, the BBB formation is done.
I am not a OB/GYN or a ped, but I assume mechanical constraints due to crossing the birth canal and bone physiology (progressive calcification of the bone matrix) has to do with this feature.
Gentle reminder, please stick your claims or rationale to the topic with citations. You are free to make your claim, but you will have to show evidence that it is somehow sound with direct citations.
LikeLike
https://www.sciencedirect.com/science/article/pii/S0946672X17300950
Will you please tell me what you think about this article?
Thank you
LikeLike
Well, I have a post about that (you can find it in my blog) and here are the two main issues: 1. You can only use the HED formula stipulated by Lyons-Weiler ONLY if you know the average plasma concentration for a defined dose.
2. Lyons-Weiler considered that an IM route is strictly equal to an IV route. Any pharmacokinetic expert would have slammed down his paper because he did not factored in the bioavailability of the IM route. In my post, using his own data he used, I show how bad his knowledge of Pharmacokinetics are.
LikeLike
[…] has explained how aluminum adjuvants are not crossing the blood-brain barrier. He has explained how polysorbate 80 works in vaccines. And he has addressed many of the studies published by Shaw, Exley, and others […]
LikeLike
[…] of aluminum, as did an actual blood brain barrier scientist and yours truly. He also wrote a very good deconstruction of the claim that polysorbate 80 breaks down the blood-brain barrier, complete with a list of many […]
LikeLike