
Preface:
This post constituted a direct response I had to the article posted by VaccinePapers.org in February 10 2015 (http://vaccinepapers.org/vaccine-aluminum-travels-to-the-brain/). However, it recently got a recycling on the Collective-Evolution article (written by an author from VaccinesPapers) through this post:
http://www.collective-evolution.com/2017/04/14/groundbreaking-china-study-links-immune-activation-by-vaccination-autism/
I will not focus more on the first half of this article and I am just providing with some facts about it that I discussed earlier on Facebook.
1. First paper (i exclude the CalTech thing since it is not peer-reviewed): They observed that mothers experiencing inflammation during pregnancy had higher risk of having offsprings with autism. Thats legit science. The senior author (Patterson) was (died in 2014) was a legit and recognized neuroscientist in the field of autism. This inflammation is either the result of some autoimmune disorder or infection. Thus the need to have mothers infection-free or avoid infectious diseases by keeping an updated vaccine schedule.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2387067/
2. The second paper, again from the Patterson lab, show again the same conclusion, this time on rhesus monkey. It again emphasize the impact of infectious disorders on maternal gestation and the risk associated on the baby. Another good reasons for expecting mommies to keep their vaccines schedule up-to-date.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3322300/
3. Now the China study show that if you increase interleukin-6 levels in the brain (IL-6, a well-known pro-inflammatory molecule), you can induce behavioral outcomes in mice that are considered representative of the ASD. It goes in the same direction that what Patterson showed and further underline the danger of having an “overactive/boosted” immune system and its ability to cause neuroinflammation. This is a growing field as we speculate that some psychiatric (depression) and neurological diseases other than multiple sclerosis (Alzheimers, stroke) maybe aggravated or induced by an inflammation and overactive immune system.
http://www.sciencedirect.com/…/pii/S0925443912000234. Then we have the slippery slope in which CE drank the Kool-Aid of BS by “ergo post hoc” fallacy. The false association fallacy: If cars run on petrol and because cars kill pedestrians, therefore petrol kill pedestrians”. This is the BS they are doing. Since vaccination will induce a transient inflammation during the immune reaction and inflammation cause autism therefore vaccines cause autism”. Of course this was debunked but here they came back with the moving goalpost. Since thiomersal did not cause an increase in number of autism, then the anti-vaxxers moved to “then it should be formaldehyde. No? Then it should be aluminum….”
To better debunk the bogus claim brought by the VaccinePapers post, I have written a long but detailed description on what is wrong with that post. Since I had initially written down into a Word documents with elements embedded in it, this may have been some formatting issues in this post. My sincere apologizes.
In this blog post, the author primarily focuses on the vaccine aluminum nanoparticles to enter and accumulate in the brain. Using several peer-reviewed articles, the author tries to convince that aluminum nanoparticles in the vaccines are uptaken by macrophages, such macrophages are capable to enter the brain and trigger neuroinflammation.
Therefore, the message of this post is clear: vaccines contain aluminum nanoparticles, aluminum is neurotoxic, and therefore vaccines are neurotoxic. If you travel in time, back in the early 2000s, the same blog post title would have talked about ethylmercury (formulated as thiomersal) contained in some vaccines and would have cited the famous “Wakefield paper” that was just published (and will be retracted a couple of years later due to gross scientific misconduct).
The blog website “Vaccine Papers” has the following slogan “an objective look at vaccine dangers”. Is it really an objective look or it is another anti-vaccine website distorting scientific studies to make fallacious claims in order to support an anti-vaccine agenda?
The goal of this article is to analyze, criticize and debunk claims made in this article and reveal the scientific fraud of this post and raise questions about the credibility of this website as a whole. In this post, we will explain why vaccines contain aluminum, which aluminum formulation has been used and is currently used in vaccines. Then we will refute the author’s arguments by directly citing passage of the post and provide a clear discussion about it.
- How do vaccines work?
To better understand the use of aluminum in vaccines, it is important for the reader to understand some fundamental concepts of immunology and how vaccines work. In mammals, we have a particular set of blood cells that are taking care of any foreign entity entering our body. It is called the immune system. To give an analogy, you can compare the immune system to the Department of Defense and the Department of Homeland Security, ensuring that anyone coming in to the United States is not posing a threat to the country.
Immune cells are all derived from a particular set of cells residing in the bone marrow: the hematopoietic stem cells (HSCs), such cells provide all the different cell types in your blood, whether we are talking about red blood cells, white blood cells or platelets.
In the figure depicted below (source: http://textbookofbacteriology.net/adaptive_2.html), HSCs will give two major cell lineages: the lymphoid stem cells (that will give the T and B lymphocytes) and the myeloid progenitors (including monocytes and macrophages).
When a foreign agent enters the system, it will induce two different types of response. In the case of a virus, it will infect some cells (depending on the type of virus) and will trigger the expression of molecules (usually viral proteins necessary for the spreading of the virus) on the cell surface. In the case of a bacteria or any entity that has a reasonable size (one thousandth of a millimeter), the bacteria will be swallowed by macrophages circulating nearby, digested and expose some fragment of this entity on its cells’ surface.
Finally circulating foreign agents can be recognized by a particular class of lymphocytes called B cells. B cells are like “keymasters”, they harbor millions of different types of keys capable to recognize any type of fragments coming from a foreign body. These tiny fragments are called in both cases, antigens. They are made of proteins, sugar or fatty acids, depending on the nature of the pathogen.
By exposing the antigen on the surface, it attracts the attention of certain immune cells. In the case of a virus, it will attract the attention of a set of T lymphocytes called CD8 T-cells that in turn will contact another type of lymphocyte called CD4 T-cells. In the case of a bacterium, macrophages and B-cells will recruit directly CD4 T-cells. CD4 T-cells acts a commander-in-chief, it will coordinate the immune response.

It will train some immune cells to seek and destroy the immediate danger by having B-cells turning plasma cells capable to secrete antibodies. These antibodies are “keys” fitting exactly inside the antigen “key lock”. By this key-key lock interactions, plasma cells will trigger the immune response that will destroy the foreign agent and eliminate it from the body. Because of this threat, CD4 T-cells is training some naïve T- and B-cells as reservists to gain the military experience and that can be rapidly mobilized in case of a future threat.
The major caveat of this response is it takes time. It takes a couple of weeks to be up and running to fight off the infection and the immune system may forget it over time.
This is how vaccines work; we use decoys mimicking the foreign agent to train our immune system so they know the profile of this agent. In case of a real threat, they can rapidly mobilize and stop the threat. By having a immune system aware and ready to fight off the infection, it considerably limits the damage caused by an infection that for many of them lead to crippling conditions (e.g. polio, varicella….) or even death (e.g. measles, whooping cough….).
In the paragraph below, you will see a chart from the Center of Disease Control (CDC) website describing of the number of crude death rate during the 20th century:
Modern healthcare practice and medical breakthroughs (discovery of antibiotics, introduction of Salk vaccines….) introduced during the 20th century have considerably reduced the number of crude death rate in less than 100 years.
Yet, some people may argue this decrease in death rate may be inherent to the introduction of hygienist practices and refute such decrease in death rate is driven by massive vaccination campaign. To refute such claims, we are referring to a study published by the Vaccine-Preventable Disease Table Working Group published in JAMA in 2007 (http://jama.jamanetwork.com/article.aspx?articleid=209448).
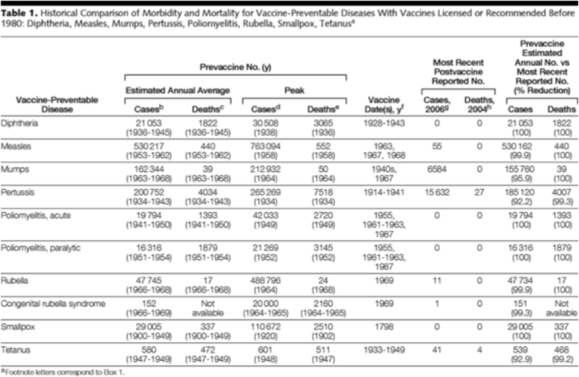
This table may appear confusing but four columns are in interests here: the pre-vaccine average number of cases and death prior the introduction of the first vaccine against the disease and the average number of cases and death as measured in 2006 and 2004 respectively. Note the dramatic decrease in number of cases and death for several of these diseases. For instance polio was a devastating disease over 70 years ago and we have zero number of cases reported. These data clearly show the potential of vaccinations. This is why vaccines are life-saving type of therapeutics and have been able to considerably reduce the number of cases if not capable to eradicate certain diseases.
However, vaccines suffer from two important caveats: Firstly, the decoys are obtained from attenuated, dead, or small bits of such infectious agents. Secondly, such decoys are by themselves are weak to induce the “immune boost” needed to provide the biological effects necessary to create the “vaccine memory”.
Therefore, these vaccines are formulated with a solution called adjuvants, that act as a “booster” to improve the immune response, resulting in a fast and bold immune response but also help to stabilize the antigen in suspension (shelf life), as well as maintaining the sterility of such vaccines (http://www.roitt.com/elspdf/Newgen_Vaccines.pdf).
Historically, the adjuvant of choice was the Freund’s adjuvant (formulation can be found here:https://www.sigmaaldrich.com/content/dam/sigma-aldrich/docs/Sigma/Product_Information_Sheet/f5881pis.pdf) but suffered from non-negligble side-effects.
Therefore a common consensus practiced in modern biomedical and clinical sciences is a gradual shift from an empirical (for instance mineral oil contained in Freund’s adjuvant has a chemical composition that is not fully known and controlled) into a synthetic (ingredients are all known and coming from primary materials with an extremely high purity) and controlled approach.
Adjuvant and formulations varies between manufacturers and between types of vaccines. The Cender of Diseases Control provides a public fact sheet detailling the composition of all vaccines currently sold in the U.S. (http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/B/excipient-table-2.pdf)
- Why is there aluminum in my vaccines? Is aluminum safe?
Aluminum (symbol element “Al”) constitutes a particular potent class of adjuvant and have shown to have a potent stimulatory effect on the immune response for over 50 years with no particular side effects or increased risk observed (for review:http://www.nature.com/icb/journal/v82/n5/full/icb200476a.html#bib1).
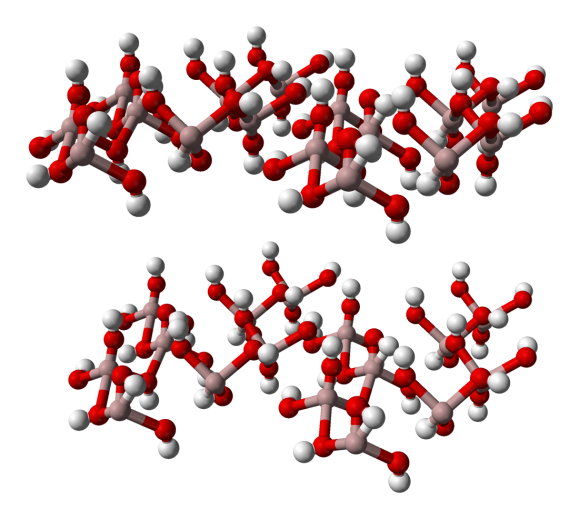
The mechanism of action of aluminum as an adjuvant remains complex and unclear. It is the third most abundant element on Earth. It is considered as a metalloid, with its ionized form being Al3+. In contact with water, aluminum undergoes a chemical reaction resulting in the formation of aluminum hydroxide (AH): 2Al + 6H2O -> Al2(OH)3 + 3H2 (dihydrogen gas).
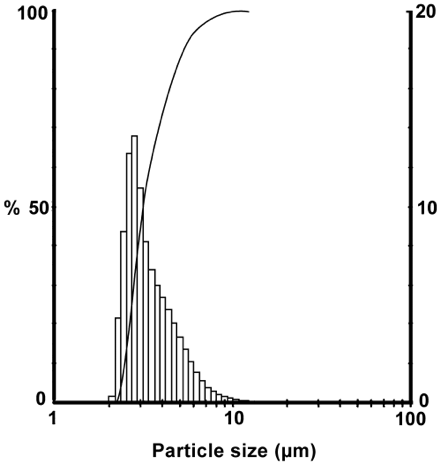
AH is classically used in adjuvants as it does not precipitate in solution, although an alternative form called aluminum phosphate (AP, AlPO4) is also used in certain vaccines formulation. This criteria is very important as chemicals used in injectable solutions have to be in an homogenous suspension. AH can organize and align themselves into crystalline structures, forming particles
Depending on how many AH are involved in these crystalline structures, these particles will have a particular sizes. In vaccines, AH particles distribution ranging from 2 to 10 micrometers, with a median size of 3 micrometer. In this post, the author refers to a particular type of aluminum, the aluminum adjuvant nanoparticles (AANs) without ever giving a bibliographical source or a definition to describe the nature of such term:
“Aluminum adjuvant nanoparticles (AANs) are transported through the body differently than ingested aluminum. Most vaccines contain aluminum adjuvant, an ingredient necessary for stimulating a strong immune response and immunity. The aluminum is in the form of Al hydroxide and/or Al phosphate nanoparticles.”
A request on search engine failed to provide us with a link on Pubmed and Sciencedirect databases with the term “aluminum adjuvant nanoparticles”, instead refers to “aluminum hydroxide nanoparticles (AHNs)” or “aluminum oxide nanoparticles (AONs)”. The usage of an uncommon term by the author is questionable and bring confusions on exactly what the author is referring to. However, the author later appears to refer to AH or AP nanoparticles, thus we speculate that AANs maybe an umbrella terms to refer to AH and APs and therefore we will refer on AHNs as AANs for the rest of this article.
Then the authors states the following: “Aluminum has been used in vaccines since the 1920s. Despite this long history, aluminum adjuvant was not studied much beyond its effect of making vaccines more effective. The safety of injected Al adjuvant was assumed, largely because aluminum is a normal (if unhealthy) component of many foods. Its one of the most common elements of the Earth’s crust. Its everywhere. So consideration of Al adjuvant safety was entirely based upon studies of ingested aluminum.” The author creates confusions for the reader as such sentences introduce a lots of concepts with few explanations and sounds more like a “word salad” than anything else.
As we have previously stated, aluminum is the third element in abundance in Earth’s crust (http://www.sandatlas.org/composition-of-the-earths-crust/). We can reasonably speculate that living organisms have been growing in an aluminum-rich environment since LUCA (last unicellular common ancestor) and therefore have adopted evolutionary traits to cope with such exposure to aluminum on the surface of Earth’s crust.
In this section, the author discussed and misused an important concept used in pharmacokinetics that will be discussed later: bioavailability. Bioavailability defines the amount of substance that reaches the systemic circulation (in other words the bloodstream) compared to the amount dispensed at the delivery site. It is a ratio of the amount measured in blood plasma following its delivery through an extravascular route (oral ingestion, intramuscular injection, dermal patch….) divided by the amount measured in blood plasma following a delivery through vascular route (most of the time an intravenous (IV) injection). When you inject a substance by IV route, this ratio is by definition 100%. Now if I re-use the example of the author, the bioavailability by oral route is 0.3%. If a patient swallows 100g of aluminum (Al), only 0.3g will make it inside the systemic circulation, thus giving us a bioavailability of 0.3%.
Although the author will cite an article by Flarend and colleagues (http://www.sciencedirect.com/science/article/pii/S0264410X97000418) later in his post, it failed to report the bioavailability reported by the same study. By courtesy, we introduce this study in this section to bring clarity. In this study, Flarend et al measured the pharmacokinetics of AH in rabbits, using radioactive aluminum (as radioactive-based analytical methods are the method of choice to quantify metals). In this study, they injected two rabbits with an intramuscular injection of AH at a concentration of 13.24 mg/mL. In an equivalent dose, each rabbit got “vaccinated” with 0.85mg of AH. According to the FDA guidelines, the amount of AH present in vaccines sold in US have a maximal amount of 1.25mg/dose with a cumulative amount (total amount you will get from vaccines) estimated of 4.22 mg over the infant vaccination schedule (source: http://www.fda.gov/BiologicsBloodVaccines/ScienceResearch/ucm284520.htm). [UPDATE] Keep in mind that such amount does not accumulate over time and we have a clearance of aluminum taking place over time. Because an intramuscular injection is not a vascular route, the bioavailability is below 100%. The authors here estimated the amount absorbed over 28 days to be 17%. What does it means? The amount absorbed is the amount that was able to diffuse through the epithelial barrier or from the connective tissue into the bloodstream (systemic circulation). It also means that 82% of the Al is still present at the site of injection (take note, AVers: if it does not absorbed, it is not absorbed). So why is that? Its all about solubility. This is the solubility equation:
Al(OH)3<-> Al3+ + 3OH-
It is an equilibrium equation, in which Al3+ is only soluble at its ionic form. Therefore, you need to deplete the Al3+ to dissolve the AH nanoparticles. At physiological pH, AH is practically insoluble. This drives the bioavailability of Al3+. If we consider the absorbed amount over 28 days, we can deduct that the bioavailability is about 0.6%, slightly higher than its absorption via GI tract.
Thus, AH releases its aluminum at a very slow pace but also at the very long time. This is why we have this biphasic curve after Cmax, with the second slope being more steady and explaining the long half-life of Al.
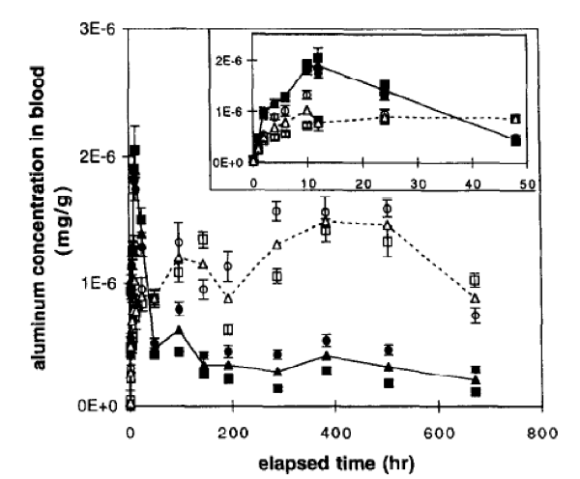
At baseline values (before injection), the amount of Al detected in plasma was about 30ng/mL. Upon injection of these four doses simultaneously, AH (black triangles) show a tmax (a time by which the concentration of aluminum peaked) at 10 hours, bringing a Cmax (maximal concentration) of 32ng/mL. In other means, a 6% increase in the amount of aluminum. Thats a bit of extra noise over noise. Not much a dramatic peak that would double up your exposure to aluminum. You don’t face an aluminum storm upon vaccine injection, but more a slight added noise over time. This is not a problem for healthy patients unless those with a kidney condition (we will discuss that later). [END UPDATE].
In the body, the authors estimated that AH mostly accumulated in the kidney, followed by the spleen and liver. This high retention is understandable as these organs are highly perfused with blood and therefore may accumulate more aluminum than other organs. These organs (liver and kidneys) are always monitored when drugs are developed as they can have serious toxic effects. However the amount accumulating is very negligible. The authors report an amount of 0.00001mg/g of tissue after 28 days. Put back into the context, at the time of injection, this tissue concentration may have peaked at 0.000283mg/g. Brain tissue, in contrast, have shown 100 times less accumulation than kidney. After 28 days, 3% of the initial aluminum injected remains in kidney, we can therefore estimate only 0.03% of the initial amount is accumulating in the brain. Aluminum has a long half-life (time to eliminate 50% of a compound from your body), as it is estimated around 100 days.
Because it takes some times to eliminate it, we can reasonably raise the question: what about the acute and chronic toxicity? The acute toxicity is defined by the toxicity obtained by a single injection, whereas the chronic toxicity is obtained from a continuous exposure.
An important concept in toxicology has been established in the 17th century by Paracelsus, the father of modern pharmacology and toxicology: “Every substance is poison, no substance is no poison. The dose and only the dose makes the substance the poison”.
It is all about how much you get exposed over time and about how long it takes to get it eliminated. A poison with a short half-life can see its toxic effect cleared very fast, whereas a poison that has a long half-live will accumulate if exposed continuously and show its toxicity after weeks if not years. This is often the case observed in poisoning with heavy metals (like lead, silver, mercury, arsenic). An historical example is Napoleon Bonaparte’s death by poisoning during his exile on the island of St. Helena. Because the amount of arsenic ingested was low and did not alter taste, it did not raise suspicion of poisoning. However because arsenic half-life is high (12 days), it kept building up in the body until it reached a toxic level.
In a review published in 2007 by Krewski and colleagues (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2782734/), non-occupational exposure to aluminum is mostly driven by food consumption, with a daily intake of 8.6 and 7.2mg/day for males and females respectively. The author of this post claim 0.3% oral bioavailabity in the following statement: “Ingested aluminum has a low absorption (about 0.3%), and when this low absorption is taken into account, there is good reason to expect vaccines to create aluminum toxicity. But that is not the subject of the present commentary. Commentary about the total amount of aluminum in vaccines can be found here: http://vaccinepapers.org/danger-aluminum-vaccines/”
[UPDATE] For our demonstration, we will rely on the data provided by the review, citing 0.1% of bioavailability. Based on this number, we can estimate males and females are exposed daily to 0.0086 and 0.0072mg/day (or 86 and 72 micrograms/day) (values were corrected for bioavailability). If we use the study from Flarend and colleagues, we should expect to add 0.21mg (or 210 micrograms) of AH per injection. Considering the 6% increase in Cmax concentration observed in rabbits following injection, we are expecting about an extra 12.6 micrograms of aluminum added to the systemic circulation. Another review by Yokel & McNamara (https://www.ncbi.nlm.nih.gov/pubmed/11322172) provides a more exhaustive comparison and sources for the amount of aluminum exposure summarized in the table below.
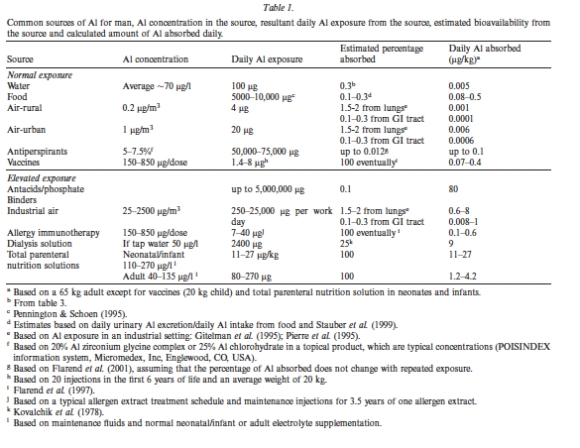
Now, we have more information available since I have written the first iteration of this post. We have an estimation of 0.07-0.4 micrograms/kg/day provided by vaccines. We will assume the more conservative number of 0.4 micrograms/kg/day. With the average weight of an infant (median weight at birth ~3.3kgs), we can assume a daily dose from vaccines of about 1.32 micrograms/day or about 237 micrograms over a 6-months period. These are plasma concentrations, therefore a better comparison would be to compare to the administration of aluminum via IV route as well.
As you can see in the chart, the most common medical procedure involving the IV infusion of aluminum is the total parenteral nutrition (TPN), or feeding directly via intravenous diffusion. The daily amount via TPN are much higher, we have values of 11-27micrograms/kg/day or for an infant getting a TPN at birth of about 36.3-89.1 micrograms/day. Therefore, the daily amount of aluminum obtained by vaccines is about 200 times less than the daily amount obtained by TPN route.
Now, this review came out before the FDA roundtable and risk assessment of aluminum in TPN bags. Following recommendation, the FDA consider an IV concentration of aluminum of 4-5micrograms/kg/day as possible neurotoxicity in premature and neonates connected to TPN bags.
Again, we have to compare to same scale. For an newborn, thats about 13.2 micrograms/day. Put the vaccine daily exposure, we are about 10% of this threshold value. Therefore, daily aluminum exposure in a vaccinated newborn infant is 10 times less the amount considered to have a possible neurotoxicity.
We have also to assume that the water and food intake does not apply to an infant and may bias our calculations. According to the Children Hospital of Philadelphia website (http://www.chop.edu/centers-programs/vaccine-education-center/vaccine-ingredients/aluminum), they estimate the total aluminum intake in infants from vaccines during the first 6 months 4.4 miligrams (thats about 4000 micrograms). This have to put into contrast from the 7 milligrams (about 7000 micrograms) from breast milk and 38 milligrams (38’000 milligrams) from formula-fed. At this point, the author is simply hand waving about the danger of aluminum by ignoring the fundamental concepts of pharmacology, pharmacokinetics and toxicology. Therefore, the question I would like to raise is why the author failed to mention the study of Flarend in this section? It constitutes the right place to discuss about it.
Now, does aluminum is harmless? Well it is all about the dose and the patients condition. Again, the review by Krewski and colleagues can bring us useful information. Al is excreted primary via kidney route, with about 95% of renal clearance. For a patient with normal kidney function, this is not a problem. For infants that receive injections on a monthly basis, this is not a problem either. The problem arises if you have a patient or a premature that have to be on a constant IV infusion, like patients on TPN bags. There is a risk of aluminum accumulation as the intake amount is much more important than the amount excreted. Such case in patients that display either immature kidneys or signs of renal failure. However, in such cases, such patients will have aluminum-depleted IV bags to avoid such accumulation. [END UPDATE]
- Aluminum and neurotoxicity
If there is a concern about aluminum toxicity, it is its possible effect on the central nervous system (we refer to it as aluminum neurotoxicity). A rapid review on Pubmed using “neurotoxicity aluminum” bring us a total number of 387 articles, including 73 reviews. A classical model to assess aluminum neurotoxicity is the model of aluminum chloride (88 articles) in rodents.
In these models, aluminum chloride (Al(Cl)3) is administered by oral route with concentration varying from 5mg/kg/day (http://www.ncbi.nlm.nih.gov/pubmed/21543463), 50mg/kg/day (http://www.ncbi.nlm.nih.gov/pubmed/25940660), with a maximal values of 200mg/kg/day as reported by Prakash and colleagues (http://www.ncbi.nlm.nih.gov/pubmed/23315010). In all these studies, anatomical changes in the brain as well as motor and cognitive functions were reported. Now, it is important to relativise these amount to a 70kg body. At the minimal concentration of 5mg/kg of Al(Cl)3, the dose-equivalent needed to achieve these neurotoxic effects would be 350mg/kg/day. Thats about more than 43 times the daily dose of aluminum obtained with food intake. Every single day. With a chronic high exposure to aluminum, we would expect to reach such toxic level. However such model is not representative as Al(Cl)3 and AH (Al(OH)3) are distinct chemical entities and therefore do not share same physical and chemical features. But this did not stop the author from making false assumptions.
“Ingested aluminum enters the blood from the gut. In the blood, ingested aluminum is in a water-soluble ionic form, typically Al3+ or an aluminum complex*. This aluminum is separated into individual atoms, like ordinary salt dissolved in water. Ionic aluminum is toxic, but it is blocked from entering the brain by the blood-brain barrier (BBB), and it is rapidly filtered from the blood by the kidneys. Unless large amounts are consumed it does not cause a problem.”
A critic I have with his statement is how the author can exclude that Al3+ cannot cross the blood-brain barrier (BBB)? I will talk about the BBB later but I wanted to mention this logical fallacy. We just discussed about the neurotoxic effects of aluminum in the CNS, using Al(Cl)3.
To better understand the difference, we have to compare the solubility of Al(Cl3) and Al(OH)3 (AH). To be soluble, a compound has to interact with water molecules and breakdown its chemical bonds to become an ion. Some can easily break their bonds (example H-Cl breaks into H+ or Cl-), some less (like H-O-H or water). Water is a polar solvent. The oxygen atom attract the electrons of the shared bonds more towards it, it then becomes electronegative. In the other hand, hydrogen discretely loses its electron and becomes slightly electropositive. Ions will mix very well because they counter the charges around. If a compound can ionize, it will dissolve in water. If it cannot ionize (like hydrocarbon chains found in oil and fat, because the carbon atom is not greedy for electrons), then it will not mix with water. That’s why oil and water never mix.
According to Wikipedia, Al(Cl)3 solubility index is 43.9g/100 mL of water and AH is only 0.0001g/100mL. In other words, Al(Cl)3 in solution is under Al3+ and Cl- forms, whereas AH remains in its Al(OH)3 form. How can the author explain the experimental studies that show the neurotoxic effects observed in animals treated with Al(Cl)3 if he claims Al3+ cannot cross the BBB?
In a section of his article, the author cites one study to disagree with it, the study of Movsas (http://www.ncbi.nlm.nih.gov/pubmed/23856981) published in JAMA Pediatrics.
“The Movsas study (published in 2013) used human infants and obtained similar results. Movsas looked for aluminum in urine and blood before and after routine vaccination with 1200mcg aluminum at the 2-month date. No change in urine or blood levels was observed. Movsas states: “No significant change in levels of urinary or serum aluminum were seen after vaccination.“ Of course, these results contradict the claims by vaccine advocates that aluminum adjuvant dissolves and is removed by the kidneys.”
An important criteria when investigating journals is the impact factor. A high impact factor is usually associated with high-quality studies as the peer-review process in such journal has a higher expectation level. In the other hand of the spectrum, we have a new category of “predatory journals” (always based on fee for publications) that will publish studies with a weak or not peer-review process. JAMA Pediatrics impact factor is fairly good (7.13) to consider the study reliable. The authors investigated the levels of aluminum before vaccination, about 11.1+/-10.3 ng/mL. Note the extreme variability of these levels among 15 pre-term babies. The author reported no changes in aluminum after vaccination and estimated to increase the concentration to 1% following the publication by Flarend (see previously). You have to remember Flarend used radioactive Al to measure the kinetics, whereas in this study, we measure aluminum using another analytical technique that may have less sensitivity. It also indicates that the aluminum contained in vaccines injection is not giving higher values than the basal aluminum level, thus you cannot distinguish the aluminum from the vaccine from the aluminum contained in food. But this important point, the author failed to understand.
Indeed, there is another study that tried to reproduce a model of vaccines injection using mice that the author surprisingly failed to cite in his report: the study of Shaw CA and Tomljenovic L published in 2013 in Journal of Inorganic Chemistry (http://www.sciencedirect.com/science/article/pii/S0162013413001773). In this study the authors tried to develop a mouse model of newborn vaccine schedule and see the effect of such repetitive doses would impact on the neurological function.

However, the experimental design is inconsistent and raises question about the validity of the data. The author never explain why they change the experimental paradigm in the low AI group. A common sense in science is when you want to show a biological effect you change one parameter at the time. For instance, the dosing schedule should stay the same, only the dose be different (as presented 50% of the normal dose) and have the control (injection with saline solution only). A poorly designed experimental setup can only to poor results and poor interpretations.

Based on this experimental setup, the authors observed an increase in weight in mice following the normal (or in this case, high) Al injections. No weight changes were observed in low AI or the control. Because of the flaw in the experimental design, we cannot tell if this effect is due to stress (remember the mice received more frequent injections than the other groups) or due to the treatment. Because of the poor experimental design, this result is worthless and resulted in an unfair use of animals to get this data. Now things become very interesting, the authors use behavioral tests for all the experiments and determined that high Al showed a decrease in the number of successful tasks. There is also a sexual dimorphism as males showed statistical differences but not females. Again, there is the experimental flaw that do not let us know if it stress related or if it is due to aluminum. In a behavioral test, you are observing your animal and try to count how many times your animal displays a movement of interest. For instance, in neurosciences, we can put a mouse into a Y-shaped maze and put a bit of cheese in one branch of the maze. Each day, you put the mouse in the bottom of the Y-maze and let the mouse find the right branch (the one containing the cheese). After 10 seconds, you will take out the mouse and score if it succeeded (1) or not (0). After scoring, you will put the mouse again in the maze and score again the mouse for 9 times, this everyday. After a few days, the mouse will remember where is the cheese and will achieve a perfect score. If the mouse has some memory problems, it will perform poorly and will maintain a low score. Now the problem is if the mouse is stuck between the two branches, do you count that as a success or a failure? That’s the problem of subjectivity. I may consider it as a success because the mouse faced the right branch, another experimenter may consider it a success only if the mouse reaches and touches the cheese.
There is also some concerns about the authors’ affiliations. Both researchers were faculty members from the University of British Columbia, Vancouver, BC (Canada) (Dept. of Ophthalmology and Visual Sciences), (Program in Experimental Medicine; Program in Neuroscience) until 2013. Surprisingly one of the authors address displayed an unusual email for an academic researcher in a public institution (cashawlab@gmail.com) but furthermore later publications saw a change in the affiliation (Neural Dynamics Research Group, 828 W. 10th Ave, Vancouver, BC, V5Z 1L8, Canada). Firstly, I would question how a faculty researcher appointed in a department in which the mission is related to eye research has the expertise to study vaccines and toxicology.
Here is the website of Neural Dynamics and surprise, we find the same authors. What is interesting, is this page has been outdated for a while and it seems funding occurred for up to 2007. Are these authors still funded? Things become more and more murky when you see the name of Stephanie Seneff (a computer scientist at the MIT that claim autism is caused…..by glyphosate….in a journal called “Entropy”) as a co-author in one the publications (http://www.ncbi.nlm.nih.gov/pubmed/25349607)……in a predatory journal! Yes, that’s what I call entropic, sorry messy publication records. Orac from “Respectful Insolence” raised a red flag on this study published earlier on and it is worth a read (http://scienceblogs.com/insolence/2011/12/08/and-global-warming-is-caused-by-the-decr/). How reliable is a peer-review from a journal aiming to publish inorganic chemistry, in assessing the validity of scientific claims that are aimed for experts in vaccines and neurotoxicology? As reliable to publish my work on the blood-brain barrier in a journal that studies plankton biology.
[UPDATE] The lab of Shaw and colleagues came again in the spotlight recently for a retracted study on the effect of HPV vaccine on behavioral issues in mice, as mentioned by Retraction Watch (source: http://retractionwatch.com/2016/02/15/journal-temporarily-removes-paper-linking-hpv-vaccine-to-behavioral-issues/). The editor-in-chief of the journal (Vaccine) did not comment about the cause of the temporary retraction. It is also worth noting that the WHO called this study on aluminum adjuvants “seriously flawed”. The full report on the WHO related to the study on the effect of aluminum adjuvant can be found here: http://www.who.int/vaccine_safety/committee/reports/Jun_2012/en/
- Aluminum nanoparticles and macrophages
Later in the post, the author discussed about how aluminum nanoparticles (AANs) can enter into macrophages as citing the following: “This model is wrong because what actually happens is that a type of white blood cell called a macrophage (MF) engulfs or “eats” (process is called “phagocytosis”) the AANs before they can dissolve. Eating foreign material is normal behavior for MFs. When MFs detect bacteria or other pathogens, the MFs engulf the pathogens, and digest them with enzymes. They then tell other immune system cells about the pathogen and how to detect it. The problem with AANs is that they are not digested by the MF enzymes. And the AANs, once inside the MF, dissolve much more slowly. The AANs persist for a long time and cause the MFs to slowly leak aluminum. MFs that consume the AANs become highly contaminated with aluminum, and spread this aluminum around wherever they go.”
Again, the author never identifies the nature of these AANs, bringing confusion to the reader. Because the author focuses on the vaccines, we speculate that he is referring to Al(OH)3 particles (AH). The author continues his explanation on why macrophages are the main cause of “MFs that consume the AANs become highly contaminated with aluminum, and spread this aluminum around wherever they go. And they go everywhere in the body.” Now the author claims these AH enter macrophages (MF), then these macrophages enter the brain and deliver aluminum across the BBB. Interestingly, after a search on Pubmed using the query “aluminum hydroxide AND macrophage”, I failed to find any relevant literature that demonstrated the inclusion of AH inside MF. Therefore the quote “Several studies show, with certainty, that MFs engulf AANs. In several studies, the AANs have been stained and photographed inside the MFs, and identified using several different methods. This is not surprising because it is well known that MFs will engulf nanoparticles just from being grown in a solution containing nanoparticles. The composition of the nanoparticles does not seem to matter“. This statement is not only exaggerated (the authors failed to provide citations to support that claim) but also provocative and fraudulent. In biological sciences, we rarely use a bold statement such as “certainty”, only when you have millions of individual records.
Only pseudoscientists would take a single study as the absolute truth.
The only study that can bring some information is the study cited by the author of this post (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4155332/) using THP-1 cells. What are THP-1 cells? THP-1 cells are monocytes derived from a patient that suffered from an acute monocytic leukemia. As any other cell line isolated from patients, these cells are readily available through cell collections such as ATCC (http://www.atcc.org/products/all/TIB-202.aspx). Technically, there are monocytes and not macrophages (see the schematics in chapter 1). Macrophages are derived from monocytes but in terms of biological identify these cells have distincts identity. It is like claiming my daughter is like my spouse. My daughter shares 50% of her DNA with my spouse and have the other 50% of mine, but she is different and unique. That simple concept appears not obvious for the author as at the end of his post cited: “Monocytes and macrophages are basically the same thing.”. Such statement is simply wrong and raises some skepticism on the rationale the author will use this study to establish his claims.
Furthermore, we have to remember that THP-1 cells are by essence a cancer cell line, they came from a patient suffering from a certain form of leukemia. Cancer cells are known to have a complete different biology than normal cells, because they are cancer cells. This is where we can start to discuss and question the validity of the authors claim: why did he not cited a study using macrophages isolated from healthy patients. The problem is there is no study that have investigated the uptake of AH by normal macrophages and we can reasonably speculate that THP-1 may have an abnormal uptake activity, resulting in an abnormal accumulation of AH.
However, there are several studies mentioning a condition called “myofasciitis”, all sharing the same co-author: Gherardi RK, the same Gherardi cited in this blog post. The author cited the following article to support the claim of AH-laden MFs: http://brain.oxfordjournals.org/content/124/9/1821. Myofasciitis (also referred as autoimmune/inflammatory syndrome induced by adjuvant) is a rare medical condition, as reported by Orphanet (http://www.orpha.net/consor/cgi-bin/OC_Exp.php?Lng=GB&Expert=592) but not listed in the Office of Rare Diseases (National Institutes of Health). The World Health Organization (WHO) provides a fact-sheet page available for information (http://www.who.int/vaccine_safety/committee/topics/aluminium/questions/en/). According to the website, it was identified in 1993 and most of the cases are located in France. Knowing that Gherardi is a French scientist currently affiliated with the Assistance Publique-Hopitaux de Paris Creteil (Department of Pathology, H. Mondor Hospital, Assistance Publique-Hôpitaux de Paris/Paris-Est University, Créteil, F-94010, France; Reference Center for Neuromuscular Disorders, H. Mondor Hospital, Assistance Publique-Hôpitaux de Paris, Créteil, F-94010, France; INSERM U955-Team 10, Créteil, F-94010, France.). The WHO teaches us two important features about the diseases:
Q1. What is MMF and how is it related to aluminium in vaccines?
- Deltoid muscle biopsies performed in France in patients with a variety of complaints have revealed in a small number the presence of a minute inflammatory focus of macrophages, along with crystal inclusions and associated microscopic muscle necrosis. These localized lesions have been shown to contain aluminium salts. Since the location of the lesions in the deltoid muscle coincides with the usual site of injection for vaccines, it would appear that these microscopic lesions are likely to be related to immunization with vaccines that contain aluminium adjuvants.
Q4. Does everyone vaccinated with an aluminium-containing vaccine have the MMF lesion?
A. Since muscle biopsies have only been carried out in patients with myopathic symptoms, there is currently no information on whether the characteristic localized histological pattern would be found in the healthy population after vaccination. It has been suggested that there might be a predisposed subset of individuals with impaired ability to clear aluminium from the deltoid muscle. Whether this reflects macrophagic dysfunction, or the tail-end of a normal population distribution of aluminium clearance and local tissue response, has not been determined.
It seems the disease is related to vaccination in patients marked by macrophages infiltration and aluminum deposition at the site of vaccination, that apparently harbor a genetic background predisposing these patients to elicit an autoimmune reaction following vaccination.
This article appears as legitimate as it shows the presence of macrophages in the muscle biopsies by tissue imaging and by using other techniques such as atomic force microscopy to quantify the amount of aluminum in such tissue samples. However, the major flaw of this paper? The absence of proper controls. There are controls documented (1252 individuals) but they never show the tissue sections from these controls or the quantification in the amount of aluminum. I found it very disturbing that such blatant flaws in the experimental design had been overseen by the peer-reviewed process, since Brain has a fairly high impact factor (IF~10).
If you inject a vaccine, you will expect an immune reaction to take place (that’s the goal of a vaccine). This translates into an inflammation stage that everyone experience few hours after injection: hot, red, swollen and painful. Inflammation also recruits a lot of macrophages (thus you would expect to see them under the microscope in your tissue samples) and you also expect to see an important amount of aluminum in the site of injection, an amount that will take time to disappear (remember the half-life of aluminum? 100 days, it takes some time to get rid of it). There is no biopsy samples from patients that have shown no side effects.
Most patients are identified in France. So there may be a rare autoimmune disease, that has a genetic background and that may be triggered by vaccines adjuvants following vaccinations. Because this condition appears only after vaccination, we may be tempted to claim vaccines caused this autoimmune disease. This conclusion is wrong as correlation is not causation. If adjuvant was causing autoimmune diseases, we should see the same condition occurring in patients not carrying the genetic mutation, with a number of cases high enough to raise some epidemiological alert. Again remember, 600 cases in France, a country that count 60 millions inhabitants.
In conclusion, although the authors theory of macrophages loaded with aluminum nanoparticles may have some scientific basis, it still remains unclear as we have almost no studies to support its claim and have a rare disease that is only documented to one country (France) and mostly by one single group (Gerhardi group). To make a claim valid, you need a high number of studies (20 and more) coming from independent laboratories and described into different parts of the world. Therefore the macrophage-loaded theory raises some skepticism and clearly contradicts the claim of “certainty” posed by the author.
- Aluminum, macrophages and the blood-brain barrier
The author claims the blood-brain barrier protects the entrance of ionized aluminum (Al3+) but completely ignored the studies showing the toxic effects using Al(Cl)3. Indeed, the author come with one esoteric theory to explain the claims: “And they go everywhere in the body. The MFs are able to travel across the blood brain barrier (BBB). The MFs, once loaded with AANs, act like a Trojan Horse and carry the AANs into the brain. This is very harmful, because the brain is very sensitive to aluminum.” Before we can talk about this theory, we have first to understand the blood-brain barrier (BBB) and how aluminum may cross the BBB.
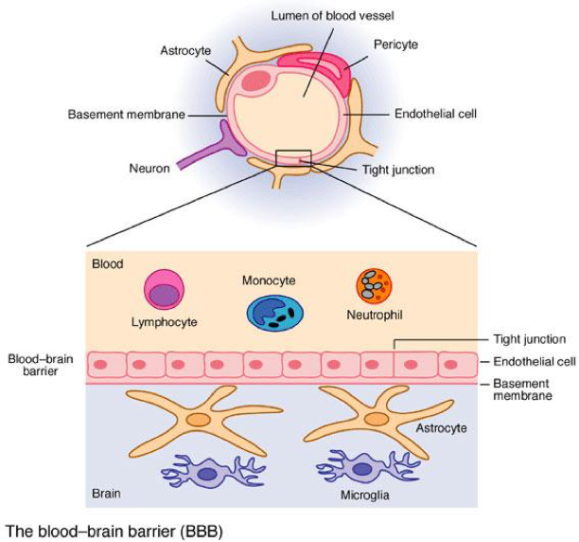
The BBB is a blood-brain interface separating the blood flow from the brain tissue (source: http://medicalterms.info/img/uploads/anatomy/blood-brain-barrier.jpg). As other blood vessels, brain blood vessels are lined by endothelial cells separating the blood flow from the brain tissue. These endothelial cells (that we usually call brain endothelial cells) are unique: they are very tight, much tighter than other vessels. Such tightness is ensured by the presence of tight junctions between endothelial cells, that block exchange of molecules as small as water and ions between the blood and the brain. These tight junctions provide a “physical barrier”. In addition to such barrier, the BBB has another type of barrier: a “chemical barrier” .
As we mentioned, if you are a small water-soluble compound (a, like sucrose (table sugar) or water), your entrance into the brain is very limited. Now if you are a chemical compound that dissolves in oil (b, lipophilic), then you can diffuse across the BBB because cells have membranes made of fat (think about biological oil droplets). However, many of the compounds are still pumped out the brain because of presence of efflux pumps. These pumps block the diffusion of toxins and also drugs (such as cyclosporin A or AZT). Indeed, these pumps are responsible in the blockade of 95% of known chemicals, either natural or synthetic. This is one of the reasons why we fail to have effective treatments for brain cancer, because our current chemotherapy drugs are blocked by the BBB and we don’t have techniques to open this barrier.
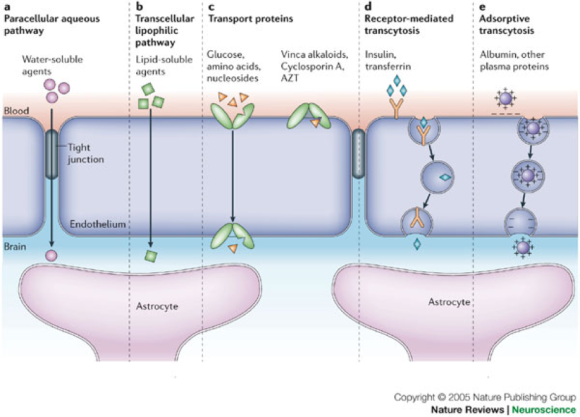
If you have a bigger cargo to deliver (like protein), it is almost impossible to deliver it across unless you have a dedicated receptor (key lock) and you have the right key to unlock it (d, receptor-mediated transcytosis). We only know a few of them, among them are insulin (insulin receptor), transferrin (transferrin receptor) and low-density lipoprotein (LDL, LDL receptor). There is an important discussion about when the BBB appears during fetal development and when do we have a mature BBB that has the function of an adult. Up to ten years ago, we believed the BBB was immature in newborns based on studies using rat and mouse pups. However, with the recent development in modern biology techniques, it seems that indeed humans have a functional BBB that maybe are as mature as adults after full term pregnancy. This was firstly supported by Saunders and colleagues that demonstrated that BBB from the opossum, a small marsupial from the same family than kangaroos and koalas, have a tight barrier (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4267212/). This observation was also observed on rat pups following stroke injury. During stroke, the BBB opens and lets water and ions enter inside the brain and causes brain damage by brain swelling. If the newborn BBB was more fragile than the adult one, the damage would be more devastating. Indeed it seems not and maybe the opposite. In a recent study, Vexler and colleagues demonstrated that rat pups better dealt with stroke injury than adult rats and showed lesser brain swelling (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3539825/).
Thus, the concept of the newborn BBB being more sensitive to vaccines than adults’ BBB maybe completely wrong. If vaccines induced BBB disruption, we should have epidemiological data showing an increase in severe neurological disorders including cerebral palsy or epilepsies. As we mentioned in the previous section, aluminum is known to show neurotoxicity, based on the Al(Cl)3 model. In this model, we speculate that Al3+ is in free form. Al3+ can bind to transferrin (a protein that normally delivers iron to the brain), thus using the transferrin receptor as an entrance mechanism (http://www.ncbi.nlm.nih.gov/pubmed/7580055). Indeed, there is little or no studies that investigated if Al(OH)3 can enter the BBB. One possible mechanism is that aluminum may disrupt the BBB, which in turn induce a BBB leakage and brain damage. The only study found is from Wiesnieski and colleagues (http://www.ncbi.nlm.nih.gov/pubmed/3730864) that investigated the effect of Al(Cl)3 and Al(OH)3 on rat BBB using radioactive sucrose to follow changes in the barrier tightness. The authors noted an increase in BBB leakage 2 and 4 hours after administration but did not show any differences after 24 hours. More interestingly, Al(Cl)3 triggered such leakage whereas Al(OH)3 showed no difference on the BBB. This study therefore refutes the idea that AH cross the BBB and/or induces BBB breakdown.
However, the author believes in the AH-loaded macrophages theory and made the following claim: “The MFs are able to travel across the blood brain barrier (BBB). The MFs, once loaded with AANs, act like a Trojan Horse and carry the AANs into the brain. This is very harmful, because the brain is very sensitive to aluminum.”
This claim is fairly outrageous for the BBB expert that I am, for different reasons. Firstly, the author simply ignores the notion of “immune privilege” organ such as the brain (for review: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3597357/). In the difference of other organs, the brain has no immune cells residing inside healthy patients. Only one type of cells, microglial cells (derived from monocytes), is the only immune cell residing inside the brain. Immune cells (including lymphocytes and macrophages) cannot enter the brain because they don’t have the right keys to open the BBB. Immune cells only cross the BBB following certain neurological disorders such as stroke or multiple sclerosis. In such diseases, brain endothelial cells undergo a phenomenon called “endothelial cell activation”, resulting in the expression of cell adhesion molecules (for review: http://www.ncbi.nlm.nih.gov/pubmed/20946472).
Following this activation, now immune cells (also known as leukocytes), have anchor points to anchor at the surface of the BBB as displayed in the schematics below. Leukocytes get anchored, undergo a complicated tango dance with the activated endothelial cells, squeeze through the endothelial cells (by diapedesis) and finally enters inside the brain. Because the brain is an “immune-privileged system”, these immune cells identify antigens present in the brain as foreign agents and triggers an neuroinflammation. A poster child of such neuroinflammation is multiple sclerosis. Therefore macrophages can only enter the brain, if you have have an activation of the BBB that will allow these cells to bind to the endothelial cell surface.
To support the claim that Al-loaded MFs are causing a neuroinflammation, the author goes again with another study from Gherardi again (remember the previous article missing the proper controls?). This time, he uses another study looking at the effect of fluorescent latex beads surface-coated with AH and published in BMC Medicine (IF~7) (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3616851/). Before we further investigate this paper, it is important to note that BMC has been recently caught in a massive fraud scale involving fake peer-reviews and the subsequent retraction of 43 papers (http://retractionwatch.com/2015/03/26/biomed-central-retracting-43-papers-for-fake-peer-review/)
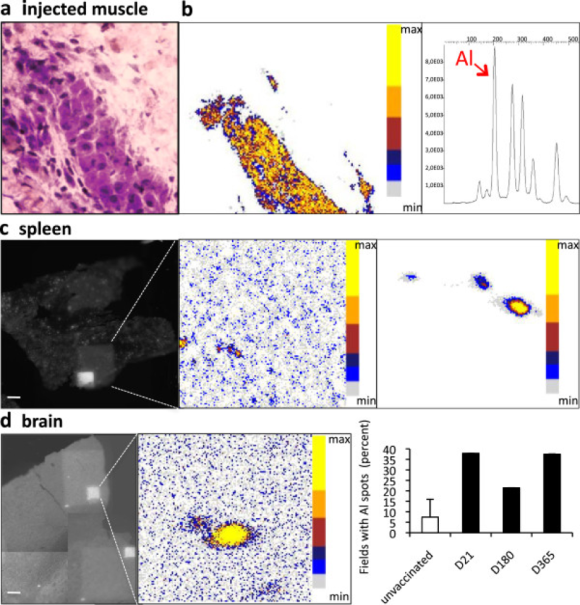
The author used the following image figure to claim the presence of aluminum inside the brain section. What appears disturbing is the inconsistency of the panel presented. On panel a, the author show a muscle biopsy tissue sample using hematoxylin-eosin staining, a common mixture of chemical dyes to observe tissue samples under a light microscope. Then for the spleen and the brain, the author show fluorescence tissue sections. Why did the authors switch from technique to another? Then we have the pseudo-colored pictures showing aluminum deposition. For the injected muscle, we can see some accumulation of aluminum consistent with the macrophages (deep purple) staining. But we cannot associate the aluminum deposition with the tissue sections of spleen and brain. Therefore nothing proves to me that the aluminum deposition observed in the spleen and brain are consistent with the presence of macrophages in that region. Also the aluminum analysis fails to show a proper scale bar. I cannot tell if panel b, c and d used the same magnification. For a manuscript of such caliber, it is unacceptable. Finally, the bar graph on the bottom right is not annotated properly. What tissue are we measuring aluminum levels over time? Muscle? Spleen? Brain?
This is the figure annotation: “Aluminum deposits in tissues following injection of alum-containing vaccine in the TA muscle. a) Granuloma composed of PAS+ cells is formed in the injected muscle envelope; b) PIXE mapping shows muscle Al deposits in pseudocolors, with confirmatory Al emission spectrum (d21); c) Section of spleen tissue (left panel) displays the large 500 × 500 μm and restricted 100 × 100 μm protonized fields corresponding to the PIXE maps (middle and right panel, respectively) enclosing eligible Al spots (d21); d) Section of brain tissue (left left panel) displays the restricted 100 × 100 μm protonized field corresponding to the PIXE map (middle panel) enclosing eligible Al spot (d21); the number of fields containing one or more Al spots was increased at all tested time points compared to unvaccinated (right panel) mice. (bars: 100 μm). d, day; PIXE, particle induced X-ray emission, TA tibialis anterior.”
We have been just at figure 1 and we have already the same botched and neglected experimental paradigm that not only make the results inconclusive but also a complete waste of animals for the experiment. A complete opposition to the author’s claim as “In an impressive study in mice, AANs and other nanoparticles (e.g. latex) were injected intramuscularly into mice”. It is not impressive; it is a deeply flawed study that anyone holding a Ph.D. degree would be outraged to read. An important point to note: I never found information on how many mice have been used for the study. The minimum required to perform statistical analysis in animal models is 8 mice per group or treatment. Therefore, I call this study as “n=1” or a single mouse study. A single individual study has no scientific value unless it is a clinical case report (however, a case report remains the lowest level in the pyramid of scientific evidence).
In the next part of this study, things become even murkier. The authors now use fluorescent latex beads (FLB) to model alum agglomerates. This is something very important. Latex and AH are completely two different chemicals. Latex is a natural polymer made of number of cis-isoprene repeats (http://www.learnnc.org/lp/media/uploads/2008/09/polyisoprene1.png). It is basically a series of repeat of a molecule made of carbon and hydrogens atoms. These are two distinct structures and FLB cannot model AH. Furthermore, why did the authors not inject AH-loaded macrophages? even AH-loaded THP-1? So instead of investigating AH accumulation in the brain, we are now having a paper that investigates the accumulation of latex particles inside the brain. Latex is a natural product that is biodegradable. Such degradation is ensured by micro-organisms (http://www.wiley-vch.de/books/biopoly/pdf/v02_kap10.pdf). Animals do not have the enzymatic toolkit to degrade latex. Latex beads will accumulate in our body. The information in Figure 2 is basically telling us we are accumulating latex beads in the site of injection and because latex is not synthesized by our cells, it is recognized as a foreign agent and macrophages will try to clear these beads from the injection sites by swallowing them.
we are accumulating latex beads in the site of injection and because latex is not synthesized by our cells, it is recognized as a foreign agent and macrophages will try to clear these beads from the injection sites by swallowing them.
In Figure 3, we are seeing the accumulation of FLB inside the brain. This is a natural consequence of injecting a substance that cannot be degraded. Because of the systemic circulation, these beads will reach the circulation from the site of injection and being spread in all areas perfused by the circulatory system. At the BBB, you will expect some non-specific uptake occurring. It is called pinocytosis, as endothelial cells will form some small sacks trapping liquid from the blood side and deliver this content to the other side. This event is rare but that happens. We can also speculate that because these animals are undergoing an important inflammation, such inflammation may be sufficient to activate brain endothelial cells and to allow FLB-loaded macrophages to enter the brain parenchyma.
Now, the onset of inflammatory response at the site of injection maybe what drives the opening at the BBB. If you look at figure 6, the intravenous injection of FLB did not trigger the infiltration of the BBB, simply because you need to have macrophages to swallow these beads in order to trigger an inflammatory signal. Macrophages are rarely circulating and mostly located in tissues. Following inflammation, macrophages will migrate to the inflammatory site. Thus explaining the absence of FLB infiltration inside the brain once injected by intravenous route. Now if you have a compromised BBB (like in mdx mice), you can see an important increase of FLB detected in brain sections from mdx mice.
To conclude, this story fails to directly demonstrate that AH triggers an inflammation in healthy mice, the authors using a complete different material (latex) to make a scientific claim that has no scientific values. You cannot claim that if I observe an allergic reaction following the ingestion of apples, it can be reproduced by ingesting oranges instead. I cannot show data using oranges and claim that these results reflect what happens when you have apples!
In addition to this study, the author also cited a study that used gold silica-loaded macrophages to target brain metastasis originated from metastatic breast cancer using a study from Clare and colleagues and published in Cancer Nanotechnologies (no impact factor as it is an open-access journal) (http://www.ncbi.nlm.nih.gov/pubmed/23205151). The authors showed they can load gold-silica nanoparticles inside macrophages directly obtained from whole blood samples of their institution Blood Center. Silica is a different entity than aluminum. It is formed by silicium (Si) that can ionize into Si2+. Like AH, silicium can bind hydroxyde and form Si(OH)2 that can crystallize and form particles. Why didn’t Gherardi and colleagues perform the same approach?
Again, this is a form of cherry-picking data, because the author tries to make the analogy between AH (Al(OH)3) and silica (Si(OH)2) – remember that these are completely two different chemical entities. Second Gherardi paper, second poor experimental designed study, second misleading conclusion. Not only did the author just drank the “Kool-Aid” without questioning it, he is also clueless on whether the Kool-Aid was genuine or tainted.
- Aluminum, autism and inflammation
Until now, we have been able to breakdown and debunk one piece at the time all these studies and showed that either their data were cherry-picked by the author to support its claim or the papers are of questionable quality that let us wonder how such papers went through the peer-review process without rejection. In the last piece, the author uses a study from Vargas and colleagues (http://www.ncbi.nlm.nih.gov/pubmed/15546155) published in Annals of Neurology, a journal with a good impact factor (IF=9.97).
It is important to note, this study is not investigating if aluminum or vaccines are causing autism. It is investigating what anatomical and biological changes can be observed between autistic brains and healthy brains. The authors used brain tissue samples from 11 autistic patients characterized by an IQ less than 70. Normal IQ score ranges from 90 to 110, so we can consider these patients as borderline. They have intelligence below average but not showing severe mental retardation. There is also an association of with epileptic seizure, with ~30% of autistic patients were epilepsy-positive. This study is legitimate and fairly well designed. We have proper controls and autistic patients. Interestingly, there is an increase in GFAP (activated astrocytes) astrocytes and HLA-DR (a cellular marker expressed in antigen-presenting cells such as macrophages, dendritic cells or B-cells) in brain samples from autistic patients. This suggests the presence of brain inflammation in these patients compared to controls. The authors further investigated and measured changes in cytokines extracted from brain tissue homogenates and cerebrospinal fluid (CSF). The brain homogenates will tell us if cells produce (and maybe releases) these cytokines, whereas the CSF (a fluid in which our brain is soaked) will tell us if these cytokines are freely circulating. Cytokine measurements were done by antibody array using cell extract and patients CSF. It measures the cytokines by trapping them on a surface and then are detected by chemical reaction resulting in the formation of a dark spot. The darker and bigger the spot is, higher is the amount of cytokine. This method has the advantage to provide some information, although a more absolute method for quantification would have been a 2-D gel electrophoresis that directly identify these cytokines by their chemical structure and count the exact amount present.
You get interesting information from this table that compares the levels of various cytokines detected in the CSF from autistic versus controls.

We can clearly see very high levels of cytokines known to promote inflammation (such as IFN-gamma, MCP-1) but there are also other cytokines known to promote BBB leakage (VEGF) and other cytokines with a biological function that remains unclear (TGF-beta2, FGF-9). This is some serious study that is supported by another research group, as published by Croen and colleagues (http://www.jneuroinflammation.com/content/11/1/113).
These studies tell us that there is an inflammatory component in a certain form of autism, with experimental data that are robust and reliable. Yet, these studies is not telling us autism is caused by inflammation or if autism causes brain inflammation. Furthermore, this study do not tell us if AH causes autism or if vaccines causes autism. However, by citing such articles at the end of this tortuous and fallacious pseudo demonstration, the authors want us to follow in the following fallacy: “Vaccines contains aluminum. Aluminum induces inflammation and get swallowed by macrophages. Macrophages causes brain inflammation. Inflammation is causing autism. Therefore vaccines causes autism”. You can see that such construction is invalid, flawed and completely irrational. Correlation IS NOT causation.
[ADDED SECTION] 7. Aluminum, the blood-brain barrier and neurotoxicity
As I have mentioned, the claim that macrophages loaded with aluminum leave the injection site and migrate to the brain via the lymphatic system and enter the brain via the BBB is unfounded and not back by science. Does it mean that aluminum does not cross the BBB?
The answer is no, aluminum can cross the BBB and therefore exert a neurotoxicity. This is why the presence of aluminum from external sources such as TPN bags can be problematic for patients that have either immature kidneys (premature newborns) or present some kidney malfunction (kidney failure, patients needing dialysis).
If I have to cite an expert in aluminum and neurotoxicity, the name of Pr. Robert Yokel (University of Kentucky) comes in mind (http://pharmacy.uky.edu/faculty/ryokel/Robert-Yokel). He has an impressive track-record in terms of peer-reviewed articles (145 publications) and other documentations. You can find his studies in Pubmed (https://www.ncbi.nlm.nih.gov/pubmed/?term=aluminum+yokel)
Aluminum can enter the BBB via various mechanisms. Because aluminum is an ion, it cannot diffuse through the BBB per se, it requires the use of carriers to piggyback on. According to a study by Yokel and colleagues, the monocarboxylate transporter 1 (MCT1) might be one of these carrier (https://www.ncbi.nlm.nih.gov/pubmed/9699794).
Another study speculate the possible use of zinc-transporter (ZnT) as Song and colleagues (https://www.ncbi.nlm.nih.gov/pubmed/18786610) described a protective effect of zinc on aluminum-induced disruption of the BBB following co-administration with zinc. We can speculate a possible competition between Zn and Al for the uptake at the BBB or we can speculate a competition for the site of action. Keep in mind that such study noted a disruption of the BBB following intraperitoneal (IP route, considered similar to IV route in terms of pharmakonetics) injection that were 5 and 10mg/kg, a value 1000x and 2000x higher than the value considered by the FDA to display neurotoxic effects (5microg/kg/day).
Another name that comes in the aluminum and neurotoxicity is the name of Chris Exley from Keele University (Staffordshire, UK, you can see his profile here: https://www.keele.ac.uk/aluminium/groupmembers/chrisexley/). He has a legitimate expertise in alumium research in chemistry, but his positions and claims on aluminum neurotoxicity are not very accurate (the link between Al and Alzheimer’s Disease is mostly based on a case report from occupational exposure: https://www.ncbi.nlm.nih.gov/pubmed/24513181), fallacious (calling on the risk of aluminum as adjuvants in vaccines without providing direct evidence for the claims: http://www.sciencedirect.com/science/article/pii/S0264410X11013089?via%3Dihub), if not simply borderline conspiracy theory (https://www.ncbi.nlm.nih.gov/pubmed/25386158).
One of the most fascinating yet skeptical claim is the ability of silicon-rich water to “clear out the brain from aluminum”, according to his clinical trial published in 2013 (http://content.iospress.com/articles/journal-of-alzheimers-disease/jad121231) and promoted by “woo” website and UK tabloid (in his case, The Daily Mail) as here (http://www.dailymail.co.uk/health/article-4320406/Silicon-rich-mineral-water-new-healthy-have.html), citing brands like Fiji water and Volvic (French mineral water)
I don’t know what he calls “silicon-rich water” (in other words, silicium dioxide (SiO2) the same chemical that make sand and your electronic chips) but I am highly skeptical how this highly polarized molecule can cross the GI barrier and the BBB, trap the Al inside the brain and clear it out.
To refute his claim, I would use the data from a study by Che and colleagues that looked at the effect of chronic exposure (13-weeks) to various dioxide via oral administration in rats (http://onlinelibrary.wiley.com/doi/10.1002/jat.3125/abstract;jsessionid=57E87335BDC127B06DAB5E9DAE7BF815.f04t01).
One figure worth a thousand words, the one about brain distribution of SiO2 in the brain of males and females. 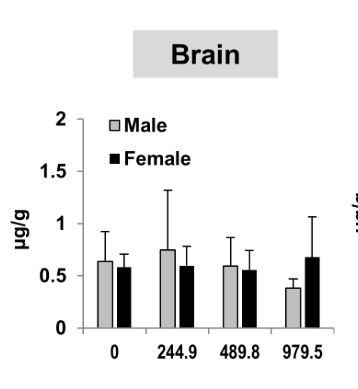
Note the dose given (mg/kg) and the dose measured in the brain (ug/g). Even by literary eating silicon (245mg/kg/day), only a bare fraction make it inside the brain (0.28% to be precise). But foremost, even at the highest amount (almost 1g/L), there is no difference between the background noise (see the control values). I would be curious how does the silicon contained in Fiji water (95mg/L) and Volvic (32mg/L) will show higher SiO2 levels when concentration 2 to 7 fold higher cannot do better than background noise. Should we assume Exley is profiteering from Big Mineral Water?
[ADDED SECTION] 8. Aluminum and infants: my comments on the “Dorea” papers
I have some comments claiming the toxicity of aluminum from vaccines, using the publications of Jose G. Dorea (Department of Nutritional Sciences, Universidade de Brasilia, Brazil). You can find his publication on that topic on Pubmed (https://www.ncbi.nlm.nih.gov/pubmed/?term=aluminum+dorea).
His research can be interesting because of the issue of soil contamination of Amazonian soil with heavy metals (lead, methylmercury, aluminum….), but also is flagged by his claims that aluminum and mercury contained in vaccines is responsible for such effects.
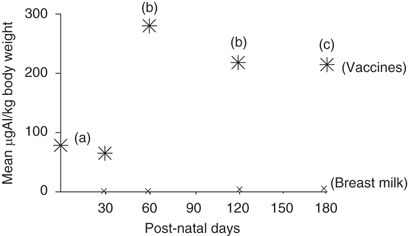
For example, I refute his claims that aluminum and mercury contained in vaccines are providing much higher levels than breastmilk from his 2009 paper because his claims are based on a flaw in data interpretations (http://www.nature.com/jes/journal/v20/n7/full/jes200964a.html?foxtrotcallback=true).
First, his claims are based on values published, not from experimental data. Therefore, he never provide experimental data for his claims and we are just speculating. Second, in the only figure of his paper, he assumes the bioavailability factor for the absorption of breastmilk but completely went south on the bioavailability of vaccines following IM or SC injection (see Figure below). If we assume the calculated bioavailability of the Flarend paper (~0.5%), then the graph looks much less impressive and completely destroy his claims. There is a big difference between 100% and 0.5% bioavailability, 200x difference.
Thats enough to bring aluminum from detectable range to potential toxic range.
We can go the same way with his other papers, they suffer the same methodological flaws: they all assume the toxic effect of Al and Hg based on hypothetical values and poor correlation, comments to studies that have nothing to do with the data presented in that study (the classical “whataboutism” and gaining one citation in Pubmed on the way, https://www.ncbi.nlm.nih.gov/pubmed/21664460). When the few times he published a paper with experimental data, he dismiss such data because it simply does not fit to his narrative. One of them is about measuring Al in infants hair, with the idea that infants who got immunized will show much higher accumulated Al levels than those not-vaccinated. Of course, the amount of Al from vaccines is marginal from Al from dietary exposure and resulted in no statistical differences. He was unhappy enough to conclude that this technique is not reliable enough. It is like trying to find patterns and hidden images in the static of an old TV (https://www.ncbi.nlm.nih.gov/pubmed/24183841).
In conclusion, I would definitely recommend not to take the Dorea’s papers as the gospel and strongly recommend anyone that has enough critical thinking and statistic literacy to not suffice with the abstract and dig in to re-analyze the data to sort the scientifically correct from the misinterpretations. There are some nuggets of interesting data in his publications but also a lot of speculations and wrong conclusions.
- Concluding remarks
In this article, we investigated, analyzed and criticized the blog post that questioned the safety of aluminum in vaccines, with an ending clearly pointed to associate autism with vaccines. The same logic can be applied to thiomersal, an adjuvant containing mercury and initially cited as a causative agent of autism following MMR study in the Wakefield study. [Correction: One reader noted the inaccuracy of this claim and I make an apology for this mistake. The retracted Wakefield paper made an association between children displaying autistic traits with MMR vaccinations (see Table 2). However, the origin (manufacturer) of such MMR vaccines was not reported and therefore such study could not pinpoint which agent contained in those vaccines was the cause of such condition. Neither such study mentioned which MMR vaccines contained thiomersal. End of correction]. Of course, the Wakefield study scientific fraud has been raised and resulted in the retraction of it. Thiomersal has been removed but anti-vaccinationists now turn to another component: aluminum hydroxide, despite the clear evidence of no association between autism and vaccines (http://www.sciencedirect.com/science/article/pii/S0264410X14006367).
Early on, we demonstrated the confusion brought by the authors. The author creates confusion by introducing the terms “aluminum adjuvants nanoparticles”. There is two class of aluminum adjuvants used in vaccines: aluminum hydroxide (AH) and aluminum phosphate. For the clarity of this article we focused on the AH nanoparticles. Unlike some websites making claims without providing any source for primary literature to support their claim, we indeed observed a smart strategic move from the author to use primary literature as sources but never showing the real data or discussing the main information coming from these studies. I call such move as a “hijack” method in which a legitimate study is used as a decoy making the claims supported by scientific evidence. A neophyte will accept this claim for granted but a more scientifically alert person will access the primary source to ensure what have been claimed on the website is in agreement with the original study. This strategy has been applied by pseudoscience websites such as “Natural-News” or “Collective-Evolution” that will have legitimate references listed to make their claims appear credible.
Another fraud observed in this post is the obvious copyright infringement by hosting and embedding PDF files of manuscripts published under conventional editorial processes. Unlike open-access journals, conventional journals requires the subscription to access their article databases. As a scientist, once my manuscript is accepted by a journal for publication, I have to secede my author’s rights to the journal. I can share the link to the abstract of my studies. If I put the PDF of the journal article on my website, freely available, I am violating the journal copyrights (you can see the copyrights information here: http://www.elsevier.com/about/company-information/policies/copyright).
However, if my studies have been funded with federal research grants (from the National Institute of Health), then my papers will be freely available through Pubmed Central after 12 months of publication embargo (I have linked to the PMC versions whenever it was possible).
Finally, we also found the few articles that were directly supporting the author claim were also the ones with questionable origin, flawed experimental setup if not suspicion of blatant scientific misconduct, even after undergoing a peer-review process.
The peer-review process has been initially designed to use the expertise of scientists to filter studies with an adequate methodology and results from those with a poor or questionable methodology. However such method is not perfect and have been subject to criticism. Even a fair and genuine peer-review in journals with the highest impact factor (Nature, Science) may fail to detect the presence of data manipulation and fabrication. If you are interested to follow on paper retraction, an excellent website to consult is Retraction Watch:http://retractionwatch.com.
We rightfully questioned several publications, all coming from two groups. An important criteria for robust scientific discovery is the ability to reproduce similar results in different laboratories, but also having such publications being reviewed in journals harboring an editorial board capable to assess the quality of your research. As a BBB researcher, trying to publish my research inside a plant biology journal may not give me the best peer-review.
Finally, statistics and certainty in science. Scientific method starts with a question (hypothesis), the design of an experiment and the subsequent outcome of such results and eventually the share of such results by publication into peer-reviewed journals. Once peer-reviewed anyone can ask to reproduce your data in their lab settings. A single study is not sufficient to qualify a phenomenon as a fact. When you have the same phenomenon that has been published a number of times by different groups and most of them show a similar outcome, we can call about a consensus. If this consensus rely on thousands of experiments that predict the same outcome each time, we can consider it robust enough to set as a theory.
In our study, we presented evidence that the additional aluminum due to vaccines injection is negligible and non-distinct from our daily exposure (food), an allergic reaction to vaccines is possible but affect so far only 1 individual per 100’000. Therefore, these individual will have a greater chance to develop such condition following massive public health campaign (for instance, France had a massive Hepatitis B vaccine campaign in 1994, which was marked by the first report of myofasciitis).
Based on the current literature, there is no evidence that AH incorporate into macrophages, such macrophages cannot enter the healthy BBB and therefore the neurotoxic effects of aluminum due to vaccines is unproven. The house of cards built by the authors just crumbled under an intense and scientific scrutiny.
In my final words, I would say to anyone trying to argue with conspiracy theorists is the same than with wrestling with a pig: you will end up exhausted, covered with mud and the pig will feel happy.

{kind=link}
{kind=link}
73 replies on “[Sciences/Junk Sciences/BBB] Aluminum adjuvants in vaccines and the blood-brain barrier. Removing the facts from the fiction, the good science from the junk science.”
Do you have any pointers on aluminum phosphate? It appears to be initially cleared at a higher rate in than aluminum hydroxide and makes alternative Al species at a slower rate (the Al rods and other agglomerates that appear inside macrophages).
LikeLike
Good Q you raise here. Indeed there is little about Aluminum Phosphate. Again nobody directly looked at Aluminum Phosphate or Hydroxide with a decent peer-reviewed paper, most of the study I have found have looked at the aluminum chloride that has a much more different physicochemical properties.
Flarend looked at both adjuvant (hydroxide versus phosphate) and I have to look at the paper to see how the PK profile look like. It is behind paywall but here is the direct link.
http://www.sciencedirect.com/science/article/pii/S0264410X97000418?via%3Dihub
LikeLike
It looks like there’s still so much work to be done in regards to safety studies on injecting aluminum hydroxide (AH) and aluminum phosphate.
But really, is it fair to label someone anti-vaccine if they do not want a product containing AH or AP to be injected into them?
LikeLike
Hi Nathan, thank you very much for your message. You see, I disagree with your claim that there is no safety studies on AH and AP as adjuvants.
We have been using these adjuvants for over 50 years, with a safety reports back from the 1970s classifying them as GRAS (Generally Recognized As Safe). If there were a problem with aluminum safety, than it would have been already identified through epidemiological data.
I would not call someone anti vaccine just because he or she does not want to have vaccines containing AH or AP, but this non-willingness to have such adjuvants in their vaccines is certainly not driven by a rationale but by misconception and fear. This can be alleviated by explaining the purpose of these, the current science of it and also dispel myths and fallacies. 99% of those arguing that AH and AP present safety issues are even based on studies that are weak, badly designed or even sometimes simply based on fallacious arguments.
Fear and science illiteracy should not be roadblocks for refusing a vaccination.
LikeLike
> Fear and science illiteracy should not be roadblocks for refusing a vaccination.
I understand what you mean there but if you step back look at vaccines as a product from a consumer point of view, aren’t they sold through fear in the first place? I just received an sms recently from the medical center “Influenza could be deadly. Get your affordable flu shot NOW”.
What do you think of Polysorbate 80 as a component in vaccines?
Are there any concerns regarding the effects of polysorbate 80 coating/binding with AH, AP or any other vaccine components that can potentially assist in crossing the BBB?
LikeLiked by 1 person
Polysorbate 80 is an emulsifier, it helps to dissolve lipid soluble compounds into aqueous solutions. To give you a practical analogy, think about dishwashing soap: it helps to clean the grease off your dishes and have them drained with the waste water. Its use in vaccines is mostly associated with the solubilization and stability of some hydrophobic antigens or lipid-soluble compounds. It seems DTaP vaccines are the one containing polysorbate. I assume it helps to stabilize the diphteria toxoid. Since AH, AP are water-soluble they would little or no interactions with the polysorbate.
For polysorbate and BBB, there are some studies out there trying to use it as a carrier (think about a Trojan horse) to deliver medicines across the blood-brain barrier. It is right now the gold rush on finding the best carrier, the best vector in drug delivery across the BBB (because it remains very hard to have anything crossed) and polysorbate 8o is one of these potential candidates to deliver medicine across.
LikeLike
First of all I hate your white text black background. Second, allow me to debunk this unscientific nonsense. Here we go:
“ For instance polio was a devastating disease over 70 years ago and we have zero number of cases reported. “
^How does this prove that engineering and water sanitation don’t also prevent polio?
____________________________________
Here’s what you said:
“Aluminum (symbol element “Al”) constitutes a particular potent class of adjuvant and have shown to have a potent stimulatory effect on the immune response for over 50 years with no particular side effects or increased risk observed (for review)”
http://www.nature.com/icb/journal/v82/n5/full/icb200476a.html#bib1
This is a wholeheartedly false statement. Al adjuvant has been linked to ASIA, immune disorders, and allergies in humans, as well as motor neuron death and precursors to Alzheimers in mice.
Here is what the paper (which is not experimental data, lol) says:
“The major source of this aluminium is apparently oral intake with food and drinking water. Martyn et al.74, based on a study in Britain, calculated the average daily intake of aluminium by humans to be 5–10 mg. Individuals with normal renal functions would excrete this aluminium uptake with the urine.”
^^so far this has nothing to do with injection of aluminum into infants.
‘ It is of interest that following injection of adjuvant containing 0.85 mg Al the normal plasma concentration of Al in rabbits (30 ng Al ml-1) only rose approximately 2 ng Al ml-1 during the experiment… Based on these figures it appears unlikely that the amount of aluminium administered via vaccination would contribute significantly to the general exposure of humans to aluminium or to the serum levels of aluminium.”
^Okay. Whatabout the concentration in the brain and soft tissues? Whatabout after 28 days? How much is left in the body? From this paper in journal of toxicology (high impact value, not cherrypicked): “Non-linear dose-response of aluminium hydroxide adjuvant particles: Selective low dose neurotoxicity”
Full paper: http://vaccinepapers.org/wp-content/uploads/Non-linear-dose-response-of-aluminium-hydroxide-adjuvant-particles-Selective-low-dose-neurotoxicity.pdf
‘Concerns about [aluminum adjuvant] safety emerged following recognition of its unexpectedly long-lasting biopersistence within immune cells in some individuals, and reports of chronic fatigue syndrome, cognitive dysfunction, myalgia, dysautonomia and autoimmune/inflammatory features temporally linked to multiple Al-containing vaccine administrations. Mouse experiments have documented its capture and slow transportation by monocyte-lineage cells from the injected muscle to lymphoid organs and eventually the brain”
^^Okay, unexpectedly long lasting biopersistence.. yet nature cites Flarend, a far less comprehensive 28 day study and only discusses plasma/serum levels. Lol. And your statement is contradicted by these researchers in this reputable, high impact journal and peer reviewed study. So. I believe them. Sorry.
Your statement:
“We can reasonably speculate that living organisms have been growing in an aluminum-rich environment since LUCA (last unicellular common ancestor) and therefore have adopted evolutionary traits to cope with such exposure to aluminum on the surface of Earth’s crust.”
^once again, nothing to do with injecting infants with aluminum. No one is saying humans don’t have a tolerance to aluminum ingestion. This is a straw man argument by you. Again.
Okay you’re moving back to Flarend again. This is a 28 day study. It is based on one single vaccine. After 28 days, 94% and 78% of Al hydroxide and Al phosphate, respectively, remained in the rabbits. If anything, this is damning for the vaccine industry. And let’s see what you have to say about it.
“Aluminum has a long half-life (time to eliminate 50% of a compound from your body), as it is estimated around 100 days.”
^^YOU LITERALLY ARE DISCUSSING A FUCKING PAPER THAT SHOWS ALIMINUM IS NOT ELIMINATED IN 100 DAYS!!! LOL!!! Okay sorry.. I just.. lol. I just … wtf!!? Maybe I am misunderstanding your statement? After 28 days 94% of ALOH remained.
Okay next thing you say “In a review published in 2007 by Krewski and colleagues (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2782734/), non-occupational exposure to aluminum is mostly driven by food consumption, with a daily intake of 8.6 and 7.2mg/day for males and females respectively.”
^^ You are talking about consumption, not injection. *sigh* common theme here. Straw man.
Anyway, I am officially bored. Seems like you should revise this .. response to vaccinepapers. I agree with some of your analysis, but most of the time it’s the same dumb straw man pharma doctor arguments I’ve heard 1 million times. Not convincing. You did not post a single experimental study that purports al adjuvant safety. You waste a lot of time discussing Flarend which is inadequate because it’s a 28 day study that does not look at the effects of the accumulation / neurotoxicity of al adjuvant. Furthermore, your analysis of Flarend is inadequate because, as stated, 94% of the ALOH3 is still In the body after 28 days. Flarend is a study on 1 vaccine and 2 rabbits. You cannot use this as a safety study for ALOH3 as you keep attempting to do.
LikeLiked by 3 people
Dear John thank you for your comment.
First, the choice of font is personal is my taste. It maybe not the best for you in your opinion, but consider it maybe worst, I could have used some weird color combinations.
I will bring this clearly and sharp, your argument that hygiene was responsible for polio eradication is simply wrong. Why?
Here are my counter-arguments:
1) The hygienist movement started in the late 19th century and early 20th century and suppose access to clean water and sewage system. Yet, the US experienced one of the worst polio outbreak before the introduction of Salk vaccine. The introduction of Salk vaccine was capable to eliminate in less than 10 years what over 50 years of public health policy could not achieve.
2) If hygienist measure was enough to eliminate polio, then it would have follow the same trend than cholera (Vibrio cholerae) outbreak. Both infectious agents are transmitted via fecal-oral contamination (usually from water contaminated by exposure to fecal matter). Cholera is always the first thing to come during a disaster when the sanitation system is lost. The last cholera outbreak in the US was reported in 1910-1911. Polio kept coming each summer until the vaccine got introduced. So why the engineering and sanitation worked to wipe cholera did not for polio?
3) The most notable example of how sanitation has nothing to do with polio? Look at India. India is certified polio-free since 2014. Yet India suffer from a major problem: the lack of toilets. Over 50% of Indian household lack the presence of a toilet system.
I am not gonna keep debunking the rest of it because you admit you are bored.
Sincerely.
LikeLike
Hi there, I would really like to hear your response to the commentators quite convincing argument that you have not proven Al adjunct safety in any way with your analysis of Flarend, and comparisons to digestive route. I found it very interesting that you came up with the % absorption via intramuscular injection and that it was that low, as I’ve been trying to find that number and without luck. Can you please give me your source? thank you for trying to clarify this topic
Celine
LikeLiked by 1 person
Hi Celine, thank you for your message. Sure, if you look at the original paper from Flarend. They estimated the bioavailability of Al (from AH) about 17% at 28 days. If we assume a zero-order kinetic based on the Al(OH3) dissolution (Al(OH)3Al3+ + 3OH-), we can conclude a daily bioavailability of 0.6%. In other words, the Al is bioavailable at a rate of 0.6% per day and eventually will become 100% over time. This matches the assumption by Yokel published in his 2001 mini-review.
https://www.sciencedirect.com/science/article/pii/S0264410X97000418?via%3Dihub
LikeLiked by 1 person
Thank you, John Clockwood, for saying everything I wanted to say to this silly “debunking” of the Vaccine Papers’ article (which clearly makes a stronger case). I would just add that the author is apparently so ignorant about aluminum that he does not know that in nature, aluminum is bound to silica and so, no, humans have not evolved over millenia with this metal in the form we now encounter it. Humans have been encountering it in the man-made form (which we now inject into our babies as well–very smart!) for only about 150 years. Watch INJECTING ALUMINUM (on Amazon) for a really fascinating look at the history of aluminum and the shoddy science supporting its safety. You’ll also get to hear a great interview with one of the world’s experts on the metal, Christopher Exley, who has been studying it for 30 years. Obviously the author of this blog has not watched the film–nor taken off his pharma blinders to objectively consider the accumulating science that supports the toxic effects of injected aluminum.
LikeLike
Hi Tasha, thank you for the comment. As usual, the best evidence Avers like you can bring is a Youtube video……maybe a New Years resolution would be to get back to college, earn some SCH in chemistry, biology and maths. You know, it helps to be scientifically literate. You will look less stupid to ask a scientist to watch a YouTube video as a peer-reviewed study.
LikeLike
Tasha. Please note that we are talking about aluminium compounds here. The most common form is aluminium oxide, not Aluminium silicate. So absolutely no-one is injecting “aluminium”. With some vaccines a tiny amount of an aluminium compound is injected subcutaneously. A wothwhile exercise is to compare that amount to the total amount any kid gets under his skin trough abrations (scratched knees) during childhood. You will see that receiving aluminium that way is ny no way new. As for Exeley, exactly what do you think makes him ” one of the world’s experts on the metal”?
LikeLike
I’ve enjoyed reading your page about aluminium. It’s very nformative. Recently I’ve noticed that a lot of anti-vaxxers seem to be switching tactics with aluminium and talking about how it causes Alzheimer’s Disease (in vaccine discussions, so still sticking with the “ooohh scary” method). I’m not sure how to respond to this – I’ve tried reading about it and have got confused. The papers seem to say that Al doesn’t cause Alzheimer’s (AD), but is elevated in patients, forms cross links in Tau proteins (apparently these proteins do get cross linked in AD), and causes tangling in the brain when injected into rabbits. I don’t know enough about AD or how Al interacts with proteins to be able to discuss it. It just feels suspect that it’s being raised in vaccine discussions (especially as I’ve come across papers making similar suggestions about AD and zinc and copper, but never a mention in vaccine discussions – probably because these aren’t used as adjuvants) – why mention a disease of old age in a discussion of childhood vaccines if not to try and frighten people?
If you ever do an update to this page, any chance you could do a paragraph on Alzheimer’s and aluminium?
LikeLiked by 1 person
Thanks for your message. The link between Alzheimers and Aluminum? Well thats a very complicated story to start with lots of low-profile studies with extreme different methods trying to link AD and aluminum. Until now, the etiology of the disease is still debated (between the Abeta team and tau hyperphosphorylation team) with at the end none that was able to break through Phase III clinical trials. In my latest (and limited knowledge), the latest clinical trial was capable to decrease Abeta plaques in patients but failed to stop the cognitive decline (http://www.reuters.com/article/us-h-lundbeck-study-idUSKCN11S2B6).
The only think that I would say about the AD and aluminum is a possible increased risk of AD and chronic exposure to aluminum (likely by occupational exposure), according to this meta-analysis. Again, in this case we can speculate that such exposure maybe driven via the intranasal route, we cannot exclude that elemental aluminum particles maybe able to cross the nasal epithelium and reach the CNS by the olfactory bulb. But thats remains to be demonstrated by some robust studies.
https://www.ncbi.nlm.nih.gov/pubmed/26592479
https://www.ncbi.nlm.nih.gov/pubmed/26247643
LikeLike
Hi!
Great writeup, but I must admit that I printed it and read it as I have an intense dislike for white on black 🙂 One additional comment and a question: While I certainly agree that Aluminium as an adjuvant probably is safe, one should be aware that it does have one irritating (no pun intended) side-effect. Studies in Sweden point to that approx 1% of those vaccinated with certain vaccines develop vaccination granulomas or an itch on the injection site. Of those approx 95% develop allegy to aluminium (PMID: 24752308 DOI: 10.1007/s00431-014-2318-2). This makes it a fairly common side-effect. My question pertains to the bioavailability of aluminium. As I understand are the mechanisms behind those granulomas and the theory of Al and autism/alzheimer completely different. The latter assumes that Al is transported in large quantities via the blood to the brain, but those granulomas are a reaction to an subcutaneous accumulation of Al at the injection site. Right?
LikeLike
Interesting point, I am trying to get access to this article but there are some points to consider:
1. If this is a complication due to aluminum-based vaccines, then we should have case reports in other geographical locations. I will check on Pubmed.
2. Trollfors have several papers investigating aluminum allergies following immunization, and recently commented in a review about vaccines adjuvants. What is interesting is that most of his references are referencing his work (that is nice but would be better if he provided any other references documenting the same type of phenomena). He also acknowledge that this allergic reaction seems to wane over time.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5214894/
3. Does granuloma share the same features than the aluminum-induced macrophage myofascitis, the famous “zebra” condition reported almost solely by Gherardi? He reported high numbers of cases in France in the mid-90s then suddenly dropped. Until now, this condition is as French as the Minitel. Could it be his “Al-induced granuloma” cases be a very rare complication restricted in a very subset of the Swedish population.
4. If this Al-induced granuloma occurs, it would interesting to follow on allergy cases in people that undergone some tattoo procedure.
A very interesting concern you raised and definitely worth a review of the literature in that regards.
LikeLike
True. Trollfors/Bergfors have researched this extensively, but there are other studies as well. I also found lots of articles describing the phenomenon in dogs 🙂 It is also true that it seems to wane over time. It is also completely possible that many cases are simply not reported as they are regarded as mild. As for #3, #4, I do not have the knowledge, but I can speculate: In my view the Al stays under the skin and seeps out slowly. In my view is it unlikely that it would enter the bloodstream in any large concentrations.
LikeLiked by 1 person
Yep, thats the point made by Flarends paper. We know Al hydroxide is not dissolving well at physiological pH. If we consider a zero-order reaction and an equilibrium reaction, then the Al as Al3+ get dissolved and reach the bloodstream, pushing the equilibrium towards complete dissolution over time. However it is slow, very slow. If we rely on Flarends data, the bioavailability (we can simplify it as the amount in bloodstream divided by the amount injected) found about 17% of injected Al particles reached the bloodstream by 28 days. Thats about 0.6% daily (if we consider a constant dissolution rate) and that explains the claim on Yokel’s review that Al will be ultimately 100% bioavailable. Thus it takes about 166 days to completely clear out this aluminum. So a very very slow release of Al. If we consider a initial amount of 1mg of Al injected, thats about 6microg that reach the bloodstream each day. We also have to consider the renal clearance into account, which is about 12.2+/-8.5microg/day. Unless you have an impaired renal function and have total parenteral nutrition (feed by IV line, in which there is a maximum recommended concentration 25microg/L), there is nothing to worry about.
LikeLike
[…] Blogger ScientistAbe published a critical review of vaccinepapers.org articles in April 2017: https://scientistabe.wordpress.com/2017/04/15/sciencesjunk-sciencesbbb-aluminum-adjuvants-in-vaccine… […]
LikeLike
I have published a rebuttal to ScientistAbe’s article: http://vaccinepapers.org/4816-2/
An important section of the rebuttal includes a list of citations supporting the fact that macrophages travel into the brain in response to inflammation (MCP-1 specifically), and that macrophages can transport substances into the brain. It is copied below. Of course, the rebuttal includes many other arguments and citations, as well.
ScientistAbe, I encourage you to address this material.
From the rebuttal:
Vargas 2005 states the following about MCP-1 in autism:
“The presence of MCP-1 is of particular interest, because it facilitates the infiltration and accumulation of monocytes and macrophages in inflammatory central nervous system disease.”
AND
“MCP-1, a chemokine involved in innate immune reactions and important mediator for monocyte and T-cell activation and trafficking into areas of tissue injury, appeared to be one of the most relevant proteins found in cytokine protein array studies because it was significantly elevated in both brain tissues and cerebrospinal fluid.”
AND
“The increased expression of MCP-1 has relevance to the pathogenesis of autism because we believe its elevation in the brain is linked to microglial activation and perhaps to the recruitment of monocytes/macrophages to areas of neurodegeneration…”
Tong et al., 2016: Monocyte Trafficking, Engraftment, and Delivery of Nanoparticles and an Exogenous Gene into the Acutely Inflamed Brain Tissue This study is particularly relevant because it showed that immune activation by lipopolysaccharide (LPS) simulated the movement of macrophages into the brain, and that the macrophages can be used to transport nanoparticles into the brain.
QUOTE: “This study was designed to fully establish an optimized cell-based delivery system using monocytes and monocyte-derived macrophages, by evaluating their homing efficiency, engraftment potential, as well as carriage and delivery ability to transport nano-scaled particles and exogenous genes into the brain…”
QUOTE: “…recruitment of circulating monocytes to the diseased sites within the CNS were evident in numerous neurological disorders [6, 14–17]. Therefore, the use of monocytes and monocyte-derived macrophages for precise therapeutics delivery still holds great promises for combating many CNS disorders…“
Brynskikh et al, 2010: Macrophage Delivery of Therapeutic Nanozymes in a Murine Model of Parkinsons Disease This paper demonstrated that macrophages can be used to deliver drugs into the brain in parkinsons disease.
QUOTE: “…we suggest the utilization of these cells [macrophages] as carriers of therapeutic formulations due to their ability to efficiently engulf particles, penetrate the BBB, and reach the site of neuropathology.”
Mello et al, 2009: http://vaccinepapers.org/wp-content/uploads/Cerebral-microglia-recruit-monocytes.pdf
QUOTE: “In conclusion, we have observed that in the setting of peripheral organ-centered inflammation there is a directed recruitment of activated monocytes into the central nervous system, which occurs as a result of an initial activation of cerebral microglia to produce MCP-1/ CCL2.” (Mello et al use “monocyte” in the broad sense, including macrophages). An important aspect of this paper is that it shows that mere inflammation-without brain injury- is sufficient to induce monocyte movement into the brain.
Choi et al, 2012: Delivery of nanoparticles to brain metastases of breast cancer using a cellular Trojan Horse
QUOTE: “More than two decades ago, Fidler and colleagues provided evidence that macrophages of blood monocyte origin can infiltrate experimental brain metastases while the blood–brain barrier is intact (Schackert et al. 1988).”
QUOTE: “The use of monocyte/macrophages as delivery vehicles to the central nervous system has been investigated in situations other than malignancy. Afergan et al. demonstrated the delivery of serotonin to the brain by monocytes, which had phagocytosed nano-liposomes containing this otherwise brain impermeant drug (Afergan et al. 2008). Dou and colleagues utilized bone marrow derived macrophages as carriers of and depots for antiretroviral drugs to treat and attenuate the symptoms of HIV-associated neurocognitive disorder (Dou et al. 2009). Therefore, we hypothesized that nanoparticle-laden monocytes/macrophages would home in to intracranial metastatic deposits by crossing the blood–brain barrier following injection into the systemic circulation.”
Batrakova et al, 2011: Cell-Mediated Drug Delivery This is a review paper on using immune cells for delivering drugs to tissues and organs (like the brain) that are normally protected.
QUOTE: “This paper reviews how immunocytes laden with drugs can cross the blood brain or blood tumor barriers, to facilitate treatments for infectious diseases, injury, cancer, or inflammatory diseases.”
QUOTE: “Immunocytes and stem cells exhibit an intrinsic homing property enabling them to migrate to sites of injury, inflammation, and tumor. In addition, they can act as Trojan horses carrying concealed drug cargoes while migrating across impermeable barriers (for example, the blood brain or blood tumor barriers) to sites of disease.”
QUOTE: “Immunocytes (including mononuclear phagocytes (dendritic cells, monocytes and macrophages), neutrophils, and lymphocytes) are highly mobile; they can migrate across impermeable barriers and release their drug cargo at sites of infection or tissue injury.”
Pang et al 2016: Exploiting Macrophages as targeted Carrier to Guide nanoparticles into Glioma / This paper describes an experiment using macrophages to transport nanoparticles into the brain, for treating brain cancers (glioma).
QUOTE: “As with other inflammatory responses, inflammation in the brain is also characterized by extensive leukocytes infiltration into brain tissue by cell diapedesis and chemotaxis [12–14]. Brynskikh et al. utilized macrophage as a drug vehicle to improve the delivery of redox enzymes into the brain for neuroprotection of dopaminergic neurons in a mouse model of Parkinson’s disease. Therapeutic efficacy of macrophages loaded with nanozyme was confirmed by twofold reductions in microgliosis and twofold increase in tyrosine hydroxylase-expressing dopaminergic neurons [15].”
QUOTE: “Inspired by these understandings, a novel strategy utilizing macrophage as a carrier to migrate across the BBB, BBTB and home into tumor sites is conceived. Importantly, macrophages are able to carry drugs into brain tumor…”
Finally, Crepeaux 2017 measured aluminum content in the brain 6 months after Al adjuvant injections. The results prove that the aluminum adjuvant winds up the brain.
LikeLiked by 2 people
Thanks for your comments. I appreciate posting some papers but it is important to read these papers rather than just gish galloping them.
I will use this reply to address them one by one.
LikeLike
Stop writing insults. I read the papers. They are relevant. They are all related and consistent, hence they are not a gish gallop. You misuse that term.
LikeLike
Vargas et al. 2005 (http://onlinelibrary.wiley.com/doi/10.1002/ana.20315/epdf).
It is an old paper but still interesting because they provide some indication of neuroinflammation component into certain forms of ASD, that has been more recently highlighted as a possible complication to pregnancy. The hypothesis that a viral, bacterial or parasitic infection contracted during pregnancy may trigger ASD in utero. A recent review by Patterson worth the read on that (https://www.ncbi.nlm.nih.gov/pubmed/21482187). They did a pretty good job at showing up signs of microglial activation and presence of reactive astrocytes and they also show evidence of increased cytokines.
This paper shows that there is a link between autism and neuroinflammation but stretching it that this was caused to vaccines is an overstatement. We also have to be careful in dealing with data when shown as mean+/-SEM as we cannot properly assess the statistics based on this (thus the push for journals to show data as Mean+SD).
LikeLike
Vargas 2005 by itself does not establish a link to vaccines. Thats what the other papers are for, including the experimental work with Al adjuvant, like Crepeaux 2017 (see link below), which reported that vaccine-relevant dosages induced microglial activation.
I cited Vargas 2005 because it stated that high MCP-1 in the brain was a notable finding in autism, and that the high MCP-1 suggests high trafficking of monocytes/macrophages into the brain in autism.
http://vaccinepapers.org/al-adjuvant-causes-brain-inflammation-behavioral-disorders/
LikeLike
What is interesting is the authors cited MCP-1 as a major chemokine upregulated in the CSF samples but did not mentioned much on IFN-gamma (that is a much more interesting pro-inflammatory cytokine well-known for neuroinflammation) and VEGF (a well-known angiogenic factor and potent BBB disruptor). MCP-1 levels were about 9-12 folds, whereas IFN-gamma was in the range of 200 fold and VEGF 81-fold increase compared to control.
They were not too much verbose on that and thats a shame.
If you look at a recent meta-analysis, IL-1beta (the classical pro-inflammatory IL) topped all of them (according to the p-value), followed by IL-6 (also known to have an contribution in neuroinflammation), IL-8, eotaxin and finally MCP-1. (https://www.ncbi.nlm.nih.gov/pubmed/24934179). Since this paper is old (12 years) it is important to also see what the most recent literature said on that regards.
If you weight all the studies included in the meta-analysis, then the contribution of cytokines is mild, there is a trend but not. There is also a gender-effect as the effect was more sustained in males versus mixed group.
LikeLike
Also see this paper, which reported that MCP-1 is elevated in serum of neonates later diagnosed with autism.
QUOTE: “We found elevated levels of MCP-1 and decreased levels of RANTES in the newborn blood of children subsequently diagnosed with ASD. ”
Of course, this implies that the infants later diagnosed with autism, because they have elevated MCP-1, will experience higher transport of Al adjuvant particles into the brain.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4080514/
LikeLike
I have one question, a very important one. Do you ever read the papers you throw at me?
This is the methods section: “Neonatal blood specimens were retrieved from the new- born screening specimen archives maintained by the California Department of Public Health. The neonatal spe- cimen archive contains dried bloodspots collected for screening purposes on nearly every infant born in California (approximately 500,000 per year) since 1980. All newborn blood specimens for children included in this study were obtained by the heel-stick method, usually within 24 to 48 hours of birth.”. So you want to tell me they were vaccinated right after being born?
This is crucial because the data points out the presence of pro-inflammatory markers right after births (<48 hours) as pointed in the discussion.
"Children with ASD were more likely to have increased levels of MCP-1 and decreased levels of RANTES in newborn bloodspots compared to GP controls. Children with DD had decreased levels of MIP-1α and RANTES compared to GP controls."
I conclude that you are keeping on gish galloping, but you also fail to recognize that you don't go through the papers per se. You cherry-pick sentences that fits to your narrative and when I am contradicting my claims based on the actual data you simply ditch as not important.
LikeLike
yes I have read all these papers.
Citing numerous papers that are on-topic and consistent is not gish galloping. Again you misuse the term.
The sentence I quoted is the first sentence in the CONCLUSIONS section.
before you go throwing more insults around, you should make sure you are getting things correct, so you dont look like a fool.
“So you want to tell me they were vaccinated right after being born?”
They likely were vaccinated immediately after being born (with Hep B vaccine), since they were born in 2000 and 2001. The Hepatitis B vaccine (which contains Al adjuvant) was recommended at birth by the CDC in 2000 and 2001. See the methods section:
“We conducted a population-based case-control study nested within the cohort of infants born from July 2000 to September 2001 to women who participated in the prenatal screening program in Orange County, California, USA. ”
The section you quote concerns the TOTAL database of samples, which extends back to 1980. But only a subset from 2000-2001 was used for this study. But thats irrelevant anyway, because…
There are two possibilities: 1) the to-become-autistic infants had elevated MCP-1 in response to the Hep B vaccine, or 2) the to-become-autistic infants had higher MCP-1 for reasons other than the Hep B given at birth.
In either case, its stands to reason that the high-MCP-1 infants will experience higher brain translocation of Al adjuvant than infants with lower values of MCP-1.
LikeLiked by 1 person
So for the Tong one, you are probably referring to this paper (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4846033/)
So here is the thing about. Figure 1, they injected these monocytes and monocyte-derived macrophages (referred as MDM) into mice treated with LPS via intracerebral injection (they used a stereotaxis table and injected into the right hemisphere). LPS is a lipopolysaccharide that has a very potent neuroinflammation induction ability. They have primed these mice into developing a neuroinflammatory state before injecting these MDM (via IV route). This is an important point to note because you need an endothelial cell activation at the BBB to allow leukocytes-endothelial interactions to happen. No neuroinflammation, no endothelial activation, no leukocytes infiltration inside the brain. Very important point to note. You need neuroinflammation, not a peripheral one to trigger that reaction.
You have to also note they have injected some bat-shit crazy amount of BK (200microg/mice that about 200microg/mL or 200microM, about 200x the amount needed to see a vasoreactivity) or mannitol (known to open the BBB via osmotic shock).
LikeLike
Your point about brain injection of LPS does not change the conclusions or implications. Tong induced inflammation in the brain, and this caused macrophage transport into the brain.
Mello 2009 used peripheral inflammation to induce monocyte transport into the brain.
Inflammation in the brain OR peripheral will induce transport into the brain.
Vaccines can do both. And aluminum adjuvant can induce inflammation in the brain.
LikeLike
Do you have any further comments regarding my rebuttal? You are welcome to comment further in the disqus thread at vaccinepapers.org
I believe a number of the arguments in your article have been shown to be wrong. Specifically, these arguments are wrong:
1) macrophages do not phagocytose or become loaded with Al adjuvant.
2) macrophages do not travel into the brain (when inflammation is present).
3) There is experimental evidence demonstrating the neurological or long term safety of Al adjuvant.
4) Al adjuvant toxicity can be predicted from models of solubilized Al3+ (released by dissolving Al adjuvant).
5) Al adjuvant does not cause brain inflammation.
6) studies shows that vaccines in general-including Al-containing vaccines-are not associated with autism.
I hope I characterized your arguments accurately in the above list. I always try to avoid making straw man arguments. Please indicate if you do not actually argue any of the above.
LikeLike
hi ScientistAbe:
Have you had a chance to read my rebuttal to your article?
I challenge you to respond to stronger rebuttal points, such as:
The cittations showing macrophages cross the BBB
The citations showing macrophages can transport substances/particles into the brain
The citations showing macrophages phagocytose Al adjuvant
The fact that Taylor 2014 is irrelevant to the safety of aluminum adjuvant (since it only includes studies of MMR and thimerosal/Hg)
The lack of safety evidence in the Lindblad 2004 paper you cited for this purpose. The lack of safety evidence in Lindblads citations.
The distinctions between Al3+ and Al adjuvant particles
The argument that there is no justification for assuming Al adjuvant toxicity is wholly explained by the released Al3+, and that the particles are biologically inert/nontoxic.
LikeLike
Hi VP, thanks for your message. I have been busy lately with my professional duties. Lets get back to your claims that macrophages/monocytes enter the brain without having a central stimulus using the Mello paper.
To keep it consistent for the readers, I am putting the URL to the paper you mention it (its the Journal of Neurosciences paper, thats a pretty good journal. Its the official journal of the Society for Neurosciences: http://www.jneurosci.org/content/29/7/2089.long).
The model used here is a hepatic bile duct resection (BDR) as well as some KO mice for different immune mediators (but thats for later). First thing first, let it be clear this is a peripheral inflammation model that is primarily aimed to induce an hepatic inflammation (the procedure is a variant of the procedure used in surgery to remove the gallbladder and redirect the hepatobiliary duct straight into the duodenum). Very important because you cannot use this model and claim “this is an inflammation stimulus similar to vaccines”.
If you look at Figure 1, you clearly see that the sham animals (underwent surgery but no bile duct ligation, thus no hepatic inflammation) have less than 1% of monocytes (CD45+/CD11b+) are found in the brain 10 days after the surgery. The BDR mice have about 6% of monocytes inside the brain. What does it tell me? It tells me that hepatic inflammation (via BDR intervention) induces monocytes infiltration. What does it not tell me? It does not tell that this phenomenon is observed in all peripheral inflammation. Hepatic inflammation is likely not inducing the same response than peripheral inflammation. Then the authors confirmed their observation and tried to understand the factors involved in such response, with MCP-1 and CCL2 being two important signaling molecules.
Then Figure 7 shows that both microglia cells and monocytes express these two factors, and in Figure 8 they show that microglial cells precede the expression of these inflammatory factors at day 5 of BDR (a timepoint by which monocytes are not inside the brain, you can see that in Fig.8A-B). The infiltration of monocytes (CD45+/CD11b+) is marginal in both sham and BDR mice. However, the number of microglial cells expressing these factors at Day 5 is significantly higher in BDR compared to sham.
What does it tell us? It tell us that you need an “inside-out” inflammation (brain-to-blood signal) to recruit monocytes. In that case, microglial cells are priming the monocytes infiltration at least by 5 days. What does it not tell us? Which mediator triggers such microglial cell activation.
We learn about one of the possible mediator in the following figures, with TNF-alpha (a common pro-inflammatory cytokine) being one factor that trigger such microglia inflammation via a TNFR1-dependent pathway (such data is supported by the use of TNFR1 and TNFR2-KO mice).
In addition the authors show that these monocytes follow the leukocyte-endothelial cell interaction pattern at the BBB as described by Pr. Britta Engelhardt (TKI, University of Bern, Switzerland. She is the expert in the BBB field for anything related to immune cell/BBB interactions), there is one review available on open-access if you are interested to read:http://www.sciencedirect.com/science/article/pii/S092544391500318X?via%3Dihub#f0010. By blocking alpha4-integrin and P-selectin (two adhesion molecules known as player in leukocytes infiltration) with blocking antibodies, the authors show that they alleviate the inflammation-induced behavioral changes due to the BDR.
The take-away from this paper (a very robust paper, but hey this is a JNeurosci paper. They have a very tough peer-review process, this is why their paper are well-designed and robust) are the following:
1) Hepatic inflammation triggers neuroinflammation with monocytes infiltration and ultimately behavioral changes.
2) This occurs with an inside-out pattern, the neuroinflammation precedes the monocytes infiltration via a TNF-alpha dependent manner.
3) Recruitment of monocytes appears mediated via a MCP-1/CCL2 dependent-mechanism.
What this paper IS NOT telling us:
1) That such response is extrapolable to any peripheral inflammation (this paper however constitutes a nice blueprint for the type of experiments to be done).
2) That vaccines adjuvants triggers a similar response in terms of inflammation amplitude. The liver is a highly perfused organ that reach the systemic circulation. Liver and pancreas inflammation are known to have some impact on the BBB. In contrast, the immunization procedure results in a more local inflammatory reaction.
3) That vaccines induce a neuroinflammation. To make this claim valid, you have to show that you have similar outcomes as observed here.
Until now, you have been making claims and put the burden on me to deconstruct your narrative. I have demonstrated, using your papers cited as evidence, that your claims are unfounded.
I will leave this post as a final comment and I will let readers make their minds but I will highlight below your argument fallacies:
1. You have been gosh-galloping me over by throwing papers asking me to rebut your claims without even spending the time to read these papers and provide your conclusions on the data shown in these papers. This is not acceptable.
2. You are making the claims, thus the burden of proof is on you. You have to deconstruct each papers and claim why they support your claims in which they are not.
3. You are guilty of using the “post-hoc ergo” fallacy by association. This is a very wrong logical assumption:
a. Vaccines cause inflammation (local though)
b. Peripheral inflammation cause monocytes infiltration inside the brain (this is true for a hepatic inflammation in mice, but yet to be demonstrated for others),
c. Thus c=a+b, vaccines cause monocytes infiltration inside the brain. This is wrong unless you show a study that has the same rigor and quality than such paper.
I am done with “feeding the troll”. I will let this comment online but I will not respond to further requests on your behalf since you are just playing various argument fallacies instead of leading a real discussion on the papers.
LikeLiked by 1 person
>>”you cannot use this model and claim “this is an inflammation stimulus similar to vaccines”.”
THATS NOT WHAT I DID. I used the Mello paper to rebut a specific false claim you made in your article: that macrophages do not cross the BBB. So stop trying to “re-write history” and falsely characterize the reasons why I cited it. Mello proves that you were wrong in claiming that macrophages cannot cross the BBB. They can, clearly, and Mello proves it.
THIS IS YOUR FALSE CLAIM:
>>”This claim is fairly outrageous for the BBB expert that I am, for different reasons. Firstly, the author simply ignores the notion of “immune privilege” organ such as the brain. In the difference of other organs, the brain has no immune cells residing inside healthy patients. Only one type of cells, microglial cells (derived from monocytes), is the only immune cell residing inside the brain. Immune cells (including lymphocytes and macrophages) cannot enter the brain because they don’t have the right keys to open the BBB. ”
So, perhaps you need to change your article.
You also claimed that macrophages do not phagocytose Al adjuvant or nanoparticles. Thats wrong, too. You are silent about that issue now, so I suppose my citations for that were effective.
The Mello paper, and others, establish that MCP-1 CAUSES macrophage transport. Therefore, the Mello results can be generalized beyond the specific hepatic injury used in the experiment: when MCP-1 is produced in the brain, macrophages travel into the brain. Further, its known that MCP-1 attracts macrophages. It has long been well established that macrophages travel towards sites of MCP-1 production. Thats why its called MCP: MACROPHAGE CHEMOTACTIC PROTEIN. DUH. Thats what MCP-1 does. It is not r surprising in any way that MCP-1 would attract macrophages to cross the BBB. It is expected, predictable.
Other experiments also support the role of MCP-1 in attracting macrophages into the brain (e.g. Khan 2013).
>>”b. Peripheral inflammation cause monocytes infiltration inside the brain (this is true for a hepatic inflammation in mice, but yet to be demonstrated for others),”
Not true. Macrophages go into the brain any time the brain produces MCP-1. Your argument that the Mello results apply only to hepatic injury are wrong.
We dont know yet if Al adjuvant induces MCP-1 in the brain, but we do know Al adjuvant and aluminum generally induce TNF-a in the brain (and TNF-a will induce MCP-1). But MCP-1 is a common chemokine and is produced in the brain in many different neurological disorders and inflammatory conditions. It is almost certain that MCP-1 is produced in the brain by Al toxicity.
>>”You are guilty of using the “post-hoc ergo” fallacy by association. ”
Thats not true because the animal experiment papers I cite are designed to establish CAUSATION.
The Crepeaux 2017 paper established that Al adjuvant injection CAUSED a large increase in Al brain content, AND CAUSED neuroinflammation (activated microglia). The Li 2015 paper showed the Hep B vaccine (which contains Al) CAUSED elevated IL-6 in the brain and caused neuro abnormalities. These experiments were designed to establish causation.
Your two arguments below are straw men, because I do not use the mello paper in this way. You erroneously describe how I use the papers I cite (you do this a lot):
>>”2) That vaccines adjuvants triggers a similar response in terms of inflammation amplitude. The liver is a highly perfused organ that reach the systemic circulation. Liver and pancreas inflammation are known to have some impact on the BBB. In contrast, the immunization procedure results in a more local inflammatory reaction.”
REPLY: I dont need to show a similar inflammation amplitude as in Mello. Immunization results in brain inflammation, in some cases. It is not always local to the injection site. Note that fever, seizure, and neurological symptoms are known to occur after vaccination.
“3) That vaccines induce a neuroinflammation. To make this claim valid, you have to show that you have similar outcomes as observed here.”
REPLY: Al adjuvant induces neuroinflammation. See Crepeaux 2017, Li 2015 and this article:http://vaccinepapers.org/aluminum-inflammation-interleukin-6/
“1. You have been gosh-galloping me over by throwing papers asking me to rebut your claims without even spending the time to read these papers and provide your conclusions on the data shown in these papers. This is not acceptable.”
You misuse the “gish gallop” term, and fail to properly understand the papers I cite. And stop throwing insults around. Insults are a refuge for incompetent people that cannot defend their beliefs.
LikeLike
I am a biochemist and virologist. I am neither pro-vaccine or anti-vaccine. I believe in pro-choice and safe vaccines. Based on our research, aluminum and mercury are toxins that cause neuroinflammation, which activate the microglia. The microglia trigger an inflammatory immune response that leads to neurodegeneration. That, in turn, depending on other pathologies, can lead to Alzheimer’s, Parkinson’s, MS and autism. Please update this post to reflect this.
LikeLike
Hi Tom. Thanks for the comments. I would be very curious to see your research and papers that back your claims. I see neurotoxicity as one thing, microglia activation as another. As far as I know, microglia is activated via two stimulus: PAMPs and DAMPs (pathogen-associated and damage-associated molecular associated pattern). Now if you bring on a couple of papers on the table that you think are relevant, then I would be more than happy to discuss and give my feedback on them “journal club -style”.
LikeLiked by 1 person
[…] Aluminum adjuvants in vaccines and the blood-brain barrier. Removing the facts from the fiction, the… […]
LikeLiked by 2 people
[…] Aluminum adjuvants in vaccines and the blood-brain barrier. Removing the facts from the fiction, the… […]
LikeLiked by 1 person
[…] be carried to the brain by macrophages. This study is well explained by Scientist Abe over at the Blood Brain Barrier Scientist. Abe is an actual scientist in neurobiology who teaches at an American university. In his post, he […]
LikeLike
You write: “The false association fallacy: If cars run on petrol and because cars kill pedestrians, therefore petrol kill pedestrians”. This is the BS they are doing. Since vaccination will induce a transient inflammation during the immune reaction and inflammation cause autism therefore vaccines cause autism”.”
It’s not analogous. Your example is more akin to saying that because needles are involved in the vaccination process, that needles therefore cause autism. Nobody’s faulting the vehicle. Yes, semantically the statement that “vaccines cause autism” is problematic. But so is the statement that “cars kill pedestrians”. What you really mean is that the actions of people in cars kill pedestrians. And what they really mean is that inflammation causes autism. That is a claim about a direct chemical cause-and-effect that be scientifically proven or disproven, but is not an inherently absurd hypothesis.
LikeLiked by 1 person
Hi Lihe,
Thank you for your comment. I (and the scientific consensus) would disagree with your statement “inflammation causes autism”. At this point, ASD main risk factor is genetic, indeed polygenic (at least dozens of genes have been identified, homozygous twins also support the genetic cause). There is a possible implication of inflammation in ASD as an environmental factor (this is supported by some data showing an higher incidence of toddlers with ASD from mothers that experienced an infectious disease during pregnancy) but this cause-and-effect still remains to be directly demonstrated.
It is an interesting hypothesis, but the way Avers are twisting and exaggerating facts make it absurd and again underline their love for the post hoc ergo fallacy.
At this point, there is no evidence that vaccines cause an inflammation high enough to trigger an neuroinflammation and subsequently certain forms of autism is not supported by robust data. I am not bringing here the HBV vaccine-neuroinflammation papers by this Chinese group because honestly it is an experimental wreck that just need a post about it by its own.
LikeLike
Hi Abe
I’m not very knowledgeable about this, so maybe you could help. A friend of says he’s concerned about the effects of mercury and aluminium in vaccines and cites this study:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3314990/
More specifically, he cites this part:
“New evidence shows that many adult mechanisms, including functionally effective tight junctions are present in embryonic brain and some transporters are more active during development than in the adult. Additionally, some mechanisms present in embryos are not present in adults, e.g., specific transport of plasma proteins across the blood–CSF barrier and embryo-specific intercellular junctions between neuroependymal cells lining the ventricles. However developing cerebral vessels appear to be more fragile than in the adult. Together these properties may render developing brains more vulnerable to drugs, toxins, and pathological conditions, contributing to cerebral damage and later neurological disorders. In addition, after birth loss of protection by efflux transporters in placenta may also render the neonatal brain more vulnerable than in the fetus.”
He puts this out as proof that any mercury or aluminium inside vaccines are dangerous to children. Any truth in this?
LikeLiked by 1 person
Hi Stix,
Thank you for the message. Glad to see some reviews by Norman (Saunders) being cited, but I guess for the wrong reasons. Norman has been a strong proponent of a functional BBB during development, before it was even cool.
Norman has been very critical of the techniques used to assess the barrier function in vivo applied to embryonic/fetal brains because the cerebral vasculature during development is more fragile than adults in terms of resilience to mechanical stress. Thats can explain the higher risk of brain hemorrhage in prematures.
Now the claims made about mercury or aluminum are inadequate because they are vague.
Lets set things straight:
First, the BBB is functional at birth. No leakiness. There are some speculation that the efflux transporters may not be fully mature, but this has more to do with lipophilic drugs (soluble in fat/oil) than hydrophilic drugs. In that case, the incidence is not much for mercury compounds (none of them appear as efflux substrates) or aluminum (it cannot diffuse the BBB as is, and the most common accepted form is likely bound to transferrin and crossing the BBB through a receptor-mediated transcytosis via transferrin receptor).
It seems not all mercury forms are equals. Yes mercury is dangerous at a certain dose, but it depends on the form and the dose applied. MeHg is usually the one raising concerns because of its bioaccumulation in tissues, especially in tissues of fish and seafood (this is why a recommendation to limit the food intake of fish and seafood is recommended). Lets take the organic forms of mercury: methyl mercury (MeHg) and ethyl mercury (EtHg) and the Burbacher study done in primates (https://www.ncbi.nlm.nih.gov/pubmed/16079072). Ignore the abstract and look at the data. You will see, for same dosing regimen, that MeHg accumulates more in the blood than EtHg, has a higher brain uptake and also a lower brain clearance.
Now for a direct comparison between both organic mercury (MeHg, EtHg) and inorganic mercury (Hg), the only study I can find is one from Hans-Joachim Galla done in vitro in porcine primary brain endothelial cell culture (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5159962/). From his data, it seems that organic mercury are diffusing across the BBB at the same rate and seems like a passive diffusion. In the opposite, the transport of Hg appears much higher than the organic forms and even seems to be polarized towards an influx.
At the end of the day, these two compounds (mercury derivatives, aluminum) are potentially neurotoxic, however their toxicity is driven by the dose and their bio persistence in the bodies.
Several studies have looked at changes in Al and Hg levels in plasma (blood) in infants after immunization (https://www.ncbi.nlm.nih.gov/pubmed/12480426 and https://www.ncbi.nlm.nih.gov/pubmed/28919482) and failed to show an elevated levels of these two metals compared to pre-immunization levels or to infants not vaccinated recently.
Unless you are living in a polluted environment (with Al or Hg values in drinking water exceeding the EPA concentrations), harboring a renal disorder (Al is cleared via renal route by 95%) or consuming an excessive amount of fish and seafood (MeHg, seems there are lots of studies about measuring levels in infants from China, Japan and Korea) during pregnancy, there is no indication of danger.
LikeLike
Also: Most, if not all vaccines are Mercury-free and has been so in large parts of the world for quite some time. There was no change in Autism prevalence when Tiomersal (An organic mercury compound) was removed.
LikeLike
Yet, 20 years later (and a fraudulent paper retracted), AVers keep beating that dead horse. Again, and again.
LikeLike
Yes. You see if the prevalence of something has increased the last 100 years, then it has to be because of the vaccines. It could not possible be because of any other change the last 100 years. That is why they keep inventing theory after theory. It was not Mercury so it has to be the aluminium, replace aluminium with something else (which might be a god idea for other reasons, but not until the replacement is proven effective) and they will focus on something else. Society has changed a lot in the last 200 years which is more than can be said about antivaxers 🙂
LikeLiked by 1 person
Yep. Society has changed a lot in 200 years, and Avers have been moving the goalposts in 200 years too, yet some think that a book published in 1889 claiming vaccines dangers with 40-years questionable statistics is still valid in 2018.
LikeLike
[…] and autism. Of course, that has also been widely discredited. You can find info on that here and here and here. Del also brings up the long-ago debunked “cdc whistleblower” nonsense. […]
LikeLike
[…] and autism. Of course, that has also been widely discredited. You can find info on that here and here and here. Del also brings up the long-ago debunked “cdc whistleblower” nonsense. […]
LikeLike
ALIMINUM IS NEUROTOXIC: In a blog post written by Professor Exley on the day his study was published, he explained the groundbreaking results:
“…while the aluminium content of each of the 5 brains [of people with autism] was shockingly high it was the location of the aluminium in the brain tissue which served as the standout observation…The new evidence strongly suggests that aluminium is entering the brain in ASD [autism spectrum disorders] via pro-inflammatory cells which have become loaded up with aluminium in the blood and/or lymph, much as has been demonstrated for monocytes at injection sites for vaccines including aluminium adjuvants.”
LikeLiked by 1 person
Groundbreaking results with a sample size of n=5 and no controls? I guess you must be really impressed quickly. What if I demonstrate you that Exley from 2017 is being shot in the foot by Exley of 2012? Check out for the update on the blog post. Using his own data provided, I will show you that Exley has served us a nothing burger. Take the average Al concentrations of his ASD brains in his 2017 study, plot it against the Al concentrations from controls samples (n=60) he published in 2012 (https://www.ncbi.nlm.nih.gov/pubmed/22045115). And even without statistics, anyone with decent basic science knowledge would laugh if you call that “irrefutable evidence” of higher levels of Al in ASD brains.
LikeLike
Hi Abe ! thanks for the post. I have just one questions regarding L.Palevski lecture, especially about nanotechnology, polysorbate and Aluminum combination. I understand that it is a nonce itself, but what is your opinion about that. haw we can reject scientifically his statement. Finally why there is no any legal issues to bring them to justice for such statements.
LikeLike
Hi Arman, thank you for your comment. I don’t know Palevski per se, but just a quick Google show me he is a “holistic medicine”. That became the new word for quack medicine.
First, nanotechnology is not even used in medicine, so why he is even concerned about? Second, trying to link PS80 and aluminum shows how Dr. Palevski needs a remediation course in organic chemistry. PS80 action on aluminum can only happen if two conditions are fulfilled: first, that aluminum particle must have a hydrophobic region capable to bind PS80. The problem is aluminum hydroxide/phopshate is a highly polar structure that is dissociating in aqueous solution. Thats not gonna work for PS80.
Second, if you have a bit of general chemistry, you came to learn about complexation and chelation. We could speculate that PS80 can chelate aluminum and help cross the BBB. However, in order to have a chelator, you need to have a chemical structure that can cage Aluminum. You need two oxygen atoms at close proximity (separated by two carbon atoms, on a cis configuration).
Lookup and compare the chemical structure of desferrioxamine (a known aluminum chelator) and PS80. You will see that PS80 is lacking the two ketone functions at close proximity needed to have the chelator effect.
Finally, for the legal issue, the problem seems to come from the medical boards. Only a medical board can strip such doctors from practicing (and even so, many will continue to practice without license. I have a quack doctor in town that is still making claims, selling supplements even after got his license revoked from the Texas Medical Board). However, the recent case that brought on some legal attention is the case of Dr. Stoller in CA.
Dr. Stoller has already a shady past, as he pushed one of his patient to undergo hyperbaric oxygen treatment in NM. I guess he fled to CA and opened an AV practice there. Unforfunately, he has been giving an unusual amount of medical exemptions in CA as a loophole to the SB277, apparently using 23andMe SNP analysis as a lab test. The city attorney of SF has requested medical records on his patients that were given medical exemptions.
https://www.northportwellnesscenter.com/practitioner/lawrence-palevsky/about
https://www.abqjournal.com/512358/doctor-accused-of-treating-child-who-wasnt-sick.html
https://www.latimes.com/local/california/la-me-vaccines-herrera-stoller-exemption-20190508-story.html
LikeLiked by 1 person
[…] He has published many studies related to these issues and also has written about them on his blog. He has explained how aluminum adjuvants are not crossing the blood-brain barrier. He has explained how polysorbate 80 works in vaccines. And he has addressed many of the studies […]
LikeLike
Dear Scientist Abe,
I have read your article very carefully and I would like to ask you some questions (please forgive my English, I am French)
– Why do you speculateabout the belief that “the living organisms have been growing in an aluminium-rich environment…” in spite of the fact that it is completely wrong to believe that, and every article on aluminium is aware of that fact: « Al was first isolated as an element in 1827, and its use as being a silvery metal began only after 1886. Al is a new metal in this context. » (Kawahara 2011 : https://www.researchgate.net/publication/50597066_Link_between_Aluminum_and_the_Pathogenesis_of_Alzheimer's_Disease_The_Integration_of_the_Aluminum_and_Amyloid_Cascade_Hypotheses)
Aluminium inhibits more than 200 important biological functions: It is always toxic, it has no biological functions whatsoever… The only “evolutionary traits to cope” with it is the gut barrier, therefore we can deal with ingested aluminium, not injected aluminium. And even ingested aluminium is very neurotoxic, very problematic for public Health: it accumulates in the brain over the years, and may be a cause for Alzheimer’s Disease.
– Why are you only referring to the Flarend study to talk about pharmacokinetics of aluminium adjuvants? Flarend is a preliminary study (the Mitkus study says so), with only 2 rabbits per adjuvant, many manipulation errors (missing samples…) and that lasted only for 28 days, a period of time way too short to observe the half-life of aluminium. Flarend was not able de determine the FORM of the aluminium he observed in the blood: you just can’t assume the aluminium was in a soluble form (Al3+) especially when you know the pharmacokinetics of aluminium adjuvants, which go through the lymph ducts, via macrophages. Aluminium adjuvants don’t dissolve, they keep their particulate form within the macrophage for a long period of time (months, years… depending on the ability to dissolve it – xenophagy)
– In fact, Flarend believed in 1997 that the aluminium he has observed in the blood (17% AH, 49% AP) was in a soluble form: it was a speculation at the time. It has been acknowledged as a big mistake since 2000 (https://www.ncbi.nlm.nih.gov/pubmed/29307441). As a matter of fact, Stanley Hem, the co-author of the Flarend study, has been confronted about this belief by the first studies presented by Pr Gherardi during the world conference on aluminium Adjuvant safety of Puerto Rico in may 2000. Stanley Hem has recognized in 2004 that the aluminium adjuvants particles had to be captured by macrophages in order to gain the lymph nodes and to create immunity. So why do you refute the macrophages capture when even the famous Stanley Hem doesn’t? No scientist working on aluminium adjuvants would dare to contradict this fact. Not in scientific literature, anyway.
– Why are you referring to studies about ingested soluble aluminium Al3+ (Yokel and McNamara 2001, Colak 2011, Singh 2015, Prakash 2013…), which are irrelevant to injected (IM) and insoluble aluminium adjuvants? Their pharmacokinetics are totally different, you can’t compare the 2 forms of aluminium. This is scientifically irrelevant and misleading, especially to your readers who are not necessarily aware of the pharmacokinetics of both aluminium forms.
– Why are you saying the Movsas 2013 study is a reassuring study, whereas it lasted only for a day? When you know the pharmacokinetics of aluminium adjuvants in the body, you know that aluminium is not dissolved. In fact, it is what Movsas observed in her study: no dissolution of aluminium adjuvants occurs in the blood and urine. The only conclusion you can make is that aluminium is not eliminated rapidly from the body. And that is not reassuring especially for infants, aluminium adjuvants stay in the body for months. If you read carefully Khan 2013, Crépeaux 2015 and 2017 (https://www.ncbi.nlm.nih.gov/pubmed/27908630), you will know that aluminium adjuvants go through the lymph ducts and therefore NOT through the blood stream. Even Flarend observed that adjuvants are not eliminated from the body (only 5,6% in a month for AH) : it is not nearly enough and very alarming for infants. Same thing for the Wisniewski study: it lasted for 24h, of course they couldn’t see any effect from the Al(OH)3 insoluble form in such a short timespan… the toxicity of Al(OH)3 is delayed, because it is not soluble, unlike aluminium chloride or lactate, which toxicities are more immediate. This error was forgivable in 1986, but not in 2017.
– Why do you believe that only Al3+ is toxic? The particulate forms are toxic too, adjuvants are not inert elements, they are very pro-inflamatory. It is a serious source of concern to know that neurotoxic fine particles can reach the infant’s brain.
– Why didn’t you read more carefully the Khan’s study, one study specifically about aluminium adjuvant distribution in the body? In fact, why do you say Khan 2013 study is about inflammation? The goal of the study was clearly to establish the biodistribution of aluminium adjuvants in the body. Why do you say we don’t know how many mice were used: it is written (3 by experiments). They discovered later that the MCP1 secretion was indeed the key factor for brain penetration. Crépeaux 2017 is about inflammation, indeed.
– Why don’t you email the researchers to ask them questions if you have some? It is how science works: asking questions.
– Why do you believe that “the dose and only the dose is the poison”? Toxicology has made tremendous discoveries during the past 20 years. Now we know that the “toxicology of fine particles” depends on the physicochemical properties of the particles (notably the size…) and the time of exposition, just like endocrine disruptors for instance. In fact, aluminium adjuvants are fine particles and the study Crépeaux 2017 observed that the lower dose was the more harmful on a short term (6 months). The higher doses could totally be harmful on a way longer term.
– You don’t seem to know how toxicology works: You made a quite surprising calculation from the Colak study, you stated 5mg/kg/day AlCl3 for a rat is equivalent to 350mg/day (not mg/kg/day) for an adult of 70 kg. Doing so, you are considering that a rat is no different than a tiny human… Why didn’t you use the allometric conversion between rats and humans (FDA Guidance 5541: the conversion between human dose to animal dose is based on the body surface area)? So you should have take the rat dose (mg/kg) and divide it by 7,4 to obtain the human dose (mg/kg).
– And above all, why do you use the AlCl3 quantities to establish the Al3+ toxic level? Don’t you know AlCl3 contains 20,2% aluminium? So we can conclude from this Colak study that a dose as small as 0,136 mg/kg/day aluminium for a human (9 mg/day for an adult of 70 kg… 0,68 mg/day for a 2-month-old baby of 5 kg…) can cause neurological problems. Fyi, at 2 months, the baby receives INFANRIX HEXA –(0,50 mg aluminium hydroxide + 0,32 mg aluminium Phosphate) + PREVENAR (0,125 mg Aluminium Phosphate) = 0,945 mg of aluminium, not excreted before months. It is a real hazard.
By the way, let’s speak about doses:
– Why don’t you give the much higher rate of Aluminium phosphate observed by Flarend, that is much more toxic on a short term than the Aluminium Hydroxide? Aluminium phosphate is present in Prevenar and Infanrix Hexa: the Mitkus study (https://www.ncbi.nlm.nih.gov/pubmed/22001122) shows that the aluminium burden from Al phosphate is even more problematic and dangerous than that of AH on a short term. If I follow your way of reasoning, you should have accrued the phosphate and the hydroxide quantities. But you didn’t. Why is that? You must know that the two kinds of adjuvants are injected to the infant on the same day.
– Why do you state that the aluminium from food (breastmilk, formulas) is more important than the one from vaccines? This is bogus. You don’t seem to have read the Mitkus study from the FDA (the only study the CDC cites as a proof of safety for infants, based on the Flarend study) or you would know that the body burden of aluminium from vaccines is higher than the one from food, for infants. The safety statement is based on the use of the ATSDR safety levels for aluminium in food (MRL 1mg/kg/day). Problem is that I’m living in France: here in Europe, the EFSA established a more drastic safety level for aluminium in food (MRL 1mg/kg/WEEK, with a NOAEL at 0,1mg/kg/day). So if I apply the European safety levels to the Mitkus study, it is quite obvious that the infant is exposed to chronic toxic levels of aluminium within the first year of life (from vaccines… but we need to also take into account the aluminium from food, obviously). It is explained in this article : https://www.sciencedirect.com/science/article/pii/S0162013417303380?via%3Dihub
– So even if we only consider the small amounts Flarend found in the blood stream, the Mitkus study (using this data) is already very alarming. But Al3+ is only one part of the problems with aluminium: the main problem is its particulate form (the dose is not the only thing that makes the poison.) That was what the Crépeaux study observed in 2017.
– To understand the exact (and very complex) adjuvant toxicity, we have to study very thoroughly the physicochemical properties of these particulate forms. Pr Exley did the work: https://aacijournal.biomedcentral.com/track/pdf/10.1186/s13223-018-0305-2
(I my opinion, you make too much ad hominem attacks: that has nothing to do with scientific methods)
– Why do you say that there is no link between vaccines and autism when even the Institute of Medecine says about the DTP, that contains aluminium : “Conclusion 10.6: The evidence is inadequate to accept or reject a causal relationship between diphtheria toxoid–, tetanus toxoid–, or acellular pertussis–containing vaccine and autism. »
https://www.nap.edu/read/13164/chapter/12#546
It is very perturbing to read you and I really wonder: if you are a BBB specialist, why do you even speak about aluminium adjuvants? You obviously don’t know anything about that very complex matter, you haven’t studied it, you haven’t read the published literature. In short, you are speculating.
Worst of all, as far as I know, you haven’t published any study on the subject in the scientific literature, and yet, you expect us to believe you against every single scientist that published actual articles on their experimental works? It is not rational. A scientist should only talk about what she/he actually studied and published on.
Every single scientist who has published articles on aluminium adjuvants safety is blowing the whistle: it is very dangerous to inject aluminium to an infant body (and some adults) especially for the neurological development. Flarend and Mitkus studies are very alarming for who knows how to read a scientific study.
Before you go that way and get tempted to brand me as an “anti-vaxxer”: I am fully vaccinated. I merely want safer vaccines for the children. Aluminium is too dangerous and people are getting wary of vaccines because of it. Do you know that aluminium is used as a placebo during clinical trials? It is not my conception of Science-Based Medicine. One exemple with the Gardasil (p.38)
https://www.scribd.com/document/367386168/V501-015-00-PRO-VD?secret_password=j4BXCUs76g4wRtDxk5cy
In the 70’s, the Pasteur Institute in France has developed another adjuvant based on Calcium phosphate that was used for 10 years without any problem in pediatric vaccines (IPAD). Calcium phosphate is a natural compound of the body. It was abandoned to aluminium when Pasteur merged with Merieux in 1984.
Click to access CTBEB.MS.ID.555585.pdf
https://www.researchgate.net/publication/308878109_Calcium_phosphate_a_substitute_for_aluminum_adjuvants
https://europepmc.org/abstract/med/4014780
Mais il semble que vous ne soyez pas du genre à remettre vos croyances en question… C’est ce qui est le plus terrifiant pour un esprit cartésien.
LikeLiked by 1 person
Hi Hypatieb,
Thank you for your message. Now that the “salamalek” were exchanged, may I ask you (or in French) that coming with your first comment in a Gish Gallop copy-pasta is not the most clever thing to be done, and tells you are a troll (le cartesien en question a identifie le commentateur en question comme un vulgaire troll). But lets go to your first point, since you are not showing sign of basic intelligence to have something to discuss on.
You said: “Why do you speculateabout [sic] the belief that “the living organisms have been growing in an aluminium-rich environment…” in spite of the fact that it is completely wrong to believe that,”
According to the CRC Handbook of Chemistry (a reference textbook for any undergraduate student that had chemistry in their curriculum), aluminum is the third most abundant element on Earth (8.23%). If we define life (and I mean any form of life from the primordial soup to as now) as made of carbon, the amount of carbon on Earth crust is so low that it is included in “all others” accounting for 0.174%. (https://chem.libretexts.org/Courses/Portland_Community_College/CH104%3A_Allied_Health_Chemistry_I_(Southeast)/3%3A_Chapter_3%3A_Atoms/3.1%3A_The_Elements).
If we assume that number was solely carbon (which is impossible), we would have about 47 atoms of aluminum for each atom of carbon on the Earth crust. Thats with large approximation and just to give a number.
You had all chance to have it correct and you just given me a stick to beat you with.
If you cannot get you CHEM101 straight by the beginning, why bother myself to read the rest of your diatribe. That was your first and last chance to troll and you will be blocked at your next comment and I will let that comment on my blog so anyone can see your sheer amount of stupid. And while you are heading back to your cave, I may suggest to listen to Georges Brassens “Quand on est con, on est con….”. You may learn a thing or two before trolling back on my page.
A bon entendeur….
LikeLike
One small comment, you say: “Do you know that aluminium is used as a placebo during clinical trials? It is not my conception of Science-Based Medicine.”
Why so? A solution with aluminium adjuvant was used for part of the Gardasil trials. For some reason, this did make some people’s underwear end up in knots, but there is a completely rational explanation for that.
When you perform clinical trials you check different things. On one hand are you interested in possible side effects. In that case you want a placebo with basically none (ie saline which was indeed used for some Gardasil trials) or a placebo where the side-effects are well known.
On the other hand are you interested in the efficacy of the vaccine, in which case the placebo arm should be as similar to the vaccine as possible, minus the active ingredient. I that case you commonly use the bare “carrier” solution which contains adjuvants and other stuff.
I can agree that Al is not ideal. There are reasons to investigate other adjuvants, but for the time being you do not want an ineffective vaccine either. I was not aware that Calcium Phosphate was used by Pasteur. Thank you for pointing that out. I will investigate further why it was abandoned.
Hope this clears up any misunderstandings you might have re clinical trials!
For the record: I am not a vaccine scientist and I am not in any way affiliated with Big Pharma.
LikeLike
Dear AndersG,
Thank you for your kind response.
I don’t question the efficacy of vaccines : the problem is the safety of vaccines. You can’t have safety trials using one of the active ingredient (and aluminium adjuvants are VERY active, they are used to activate the immune system). Aluminium is not inert, it can’t be used as a neutral placebo.
Side-effects of aluminium adjuvants are not well known : we can use the composition of the vaccine minus the antigens for an efficacy trial, why not, but not for a safety trial. That is dishonest.
Furthermore, it is not ethical to inject the aluminium adjuvant only : there is no benefit to gain for the persons involved in the control group. And we can see the side effects are the same between the “vaccine group” and the “placebo group” : we must conclude than the aluminium causes these side effects (neurological disorders and others).
That is not evidence-based Medicine.
Aluminium adjuvants are neurotoxic, the doses injected are way too important (higher than the european safety doses) especially for infants. It HAS to be removed, and we can use Calcium Phosphate.
In fact, with Calcium Phosphate, 2 doses of vaccines were enough, when 3 doses of aluminium adjuvanted vaccines were necessary : so the industry choose the most profitable adjuvant, knowing that it would be hazardous for infants and some adults (in France anyway because we have letters from Pasteur Institute that explained that to the french Health minister in 1984…)
LikeLike
But you make the assumption that we are talking about safety trials only. That is not the case. Clinical trials measure both safety and efficacy. Both are important. There is no dishonesty there.
There is no benefit either from incecting a saline placebo so your ethical argument is incorrect.
You write “with Calcium Phosphate, 2 doses of vaccines were enough, when 3 doses of aluminium adjuvanted vaccines were necessary” – What vaccine specifically? They are all different. From what I see was it used for the DTP vaccine which is a completely different vaccine from the HPV one.
Then you make several blanket statements without providing supporting evidence. Aluminium Adjuvants have known negative sideeffects, but neurotoxicity at the levels used in vaccines has never been shown to be one of them.
That being said, there is ongoing research on this matter and I am far from convinced that Aluminium is used out of pure greed. There are several articles in PubMed and a quick google turned up this study that apparently shows that CaPo is not as efficient as aluminium, nor completely safe.
http://www.ijcea.org/index.php?m=content&c=index&a=show&catid=58&id=747
LikeLike
We are talking about safety trials in fact, all of us. We don’t speak here about efficacy of aluminium adjuvants: they are very effective. Too effective I would say. Vaccines are effective, no doubt.
But aluminium adjuvants are not safe : no study can state otherwise. Even Mitkus 2011 is not a proof for doses safety.
So before saying “aluminium is safe”, the industry should be able to prove it, but it can’t. Therefore, nothing can support this claim. And many studies show the tremendous negative effects of aluminium (all the Pr Gherardi’s team work in France, or the Pr Lujan’s team in Spain, for example).
Read this study about the sheep from the spanish team : it has a true placebo VS aluminium VS vaccine groups, very interesting.
Click to access paper-yphrs-4037-201811001554587683-with-suppl-material.pdf
This study is crystal clear about aluminium neurotoxic side effects in a big mammal (sheep). So what is the effect on an infant ?
Safety trials are not the same as efficacy trials : it is obvious. Safety trials should be tested with true inert placebos, unless it is dishonest. Or is it the definition of “placebo” that has changed ? It is “a substance with no effects that a doctor gives to a patient instead of a drug. Placebos are used when testing new drugs”, isn’t it ?
Nobody can say aluminium has no effect : it is an adjuvant, it activates the immune reaction.
Calcium Phosphate was used in DTPolio and DTCPolio vaccines (IPAD). Please read this :
Click to access CTBEB.MS.ID.555585.pdf
https://www.researchgate.net/publication/308878109_Calcium_phosphate_a_substitute_for_aluminum_adjuvants
https://europepmc.org/abstract/med/4014780
Then, I agree it has to be tested for safety (Calcium phosphate is not neurotoxic).
Vaccines are given to healthy infants: safety should be the bigger concern. It is not (for many reasons), hence the ever growing suspicion. To improve vaccines, we must stop using aluminium, or vaccine rejection will keep growing.
LikeLike
I guess you show the nice troll you must be and spam my mailbox over the last 72 hours.
I gonna be nice and let you know that I will publish your comments published as of today, to showcase to other readers the anatomy of a troll and how to spot them:
1.The average troll comes to your page with a diatribe longer than a CVS receipt.
2. It will usually start with a Gish Gallop asking you to answer 20 questions to make themselves look smart.
3. The problem is the average troll does not know the lack of basic knowledge needed to argue properly. Troll came here claiming that my initial claim of aluminum being the third most abundant element on Earth crust and therefore life adapted to deal with aluminum to an extent is fallacious. Troll surely never read a chemistry textbook.
4. Troll claims he was censored and I erased his messages (see comment #3 of troll). What troll does not understand that WordPress is a private page, I have control of my page and I moderate whatever gets published. Troll must be antisocial to expect my answer with in 5 minutes but I have a life beyond my basement and deal with life/work balance. Troll got again lying and displayed his sheer stupidity.
5. Thats lead to my final comment (and final warning to troll). Troll got two strikes of caught lying, was given a warning and dogpiled me twice with his comments (see comments #2 and #3). Troll did not read my comments and just kept his diatribe.
I have no obligation to feed troll. Troll is just feeding on anger and copy-pasta from his AV playbook. Never feed a troll, let it starve from attention and troll will go.
This will be his last comment and from now on I will deal with troll like any spammer.
LikeLiked by 1 person
Another thing worth mentioning is that some people tend to attribute stuff to their opponents that said opponents never claimed. I have never claimed that Aluminium “has no effect”. It definitely has and everything that has an effect can have side effects, but supporting oneself solely on people like Gherardi, Shaw, Tomlijenovic is plainly speaking cherry picking.
Also claiming “Calcium phosphate is not neurotoxic” without providing any supportive evidence is hardly convincing. In reality Calcium ions can cause neurotoxicity given the right conditions.
LikeLike
One additional comment: Currently, only aluminium-based adjuvants are approved in the US (Tritto et al 2009) and US is a large market. That means that there is a strong business case for using them as well as a safety aspect (right or wrong one would assume that the US stance is based on science).
There is no such thing as a “safe” adjuvant. It is the same mechanisms that make them suitable as adjuvants that can cause side-effects. In the end you need to balance immune stimulation with possible side effects (Batista-Duharte et al 2011)
LikeLike
Of course not, don’t you know squalene and others adjuvants are approved too ?
https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/common-ingredients-us-licensed-vaccines
https://www.cdc.gov/vaccinesafety/concerns/adjuvants.html#as01
Is it possible not to delete my messages ?
Merci par avance.
LikeLike
I stand corrected. I was quoting a paper from 2009. The more recent FDA page gives other info. The point is still that the US is a large market and adjuvants not approved by the FDA have a very small chance of being used.
LikeLike
[…] Tech University. Abe also has a blog where he explains aluminum adjuvants, among other subjects. Herein, Abe discusses junk science (cough what Ashley shares cough) and why it is junk. As I was taught by […]
LikeLiked by 1 person
I understand that you show the bioavailability of aluminum injected into muscle tissue is higher than ingested, but I think there is one thing you gloss over. The likelyhood of accidentally injecting aluminum straight into your blood stream by eating it is near zero. What is the likelihood of a vaccine being injected incorrectly leading to a large amount in the blood stream much quicker than you researched? For all intensive purposes the values you reached are a minimum amount of aluminum in the blood stream if everything goes right. In life, things rarely go according to plan for something as complex as an injection.
LikeLike
Hi Kyle, thank you for your message. Well, your hypothesis is interesting but very unlikely. Let me explain it. First, the injection site is intramuscular. Thats a very dense tissue with very small vessels and a low number of vessels as well. Think about a steak, a nice piece of tenderloin. To imagine the challenge of perforating a vessel, think about how hard it is to marinate a piece of meat. Takes hours. Thats alreay reduce it the probability to happen, but lets say it still can happen. The next challenge you gonna get is the dissolution rate. Remember the pH by which the aluminum dissolve the least (very low Ks value)? About 7-7.5. Blood pH under physiological condition is 7.4 (+/-0.05). Get a bit too acidic (7.2) or alkaline (7.6) and you will have severe symptoms of acidosis and alkalosis respectively. I would assume that even if we have all of an aluminum injected, we will still have to face the limits of dissolution rate. The aluminum salts are inert per se. What concerns us is the amount of free aluminum (Al3+) circulating. Thats the one we are concerned about and it is very unlikely that it will dissolve faster in blood than in tissue, just by considering the pH. To also remove an issue, I would cite the paper from Weisser and colleagues. She injected IM aluminum citrate (one form found in plasma, alonsgside with transferrin-bound aluminum) that is releasing Al3+ to 100% rate within an hour. She reported no changes in Al plasma concentration either. Unless we are injecting fast-releasing forms of Al salts directly IV at huge and continuous dose (e.g. continuous infusion), the risk of having things goes wrong is very very very very small, much smaller than the risk inherent to contract a VPD.
https://www.ncbi.nlm.nih.gov/pubmed/30302509
LikeLiked by 1 person
Hi! I have been trying to put stuff in perspective and given the fact that Al is abundant and vaccinations are subcutaneous of intramuscular… The HPV vaccine for example contains 0.5mg of aluminium. The earhs crust is 7% aluminium. There is considerable variation, but for simplicity let’s assume that 1g of soil har 7% aluminium, so 0.5mg of aluminium is what we get from 7.14mg of soil. Kids fall and scratch their arms and knees and get dirt in the wounds. How much? I would guess that an average child will get quite a lot more aluminium this way, than through vaccines. Or have I missed something?
LikeLike
[…] Aluminum adjuvants in vaccines and the blood-brain barrier. Removing the facts from the fiction, the… […]
LikeLike
[…] topic, complete with listing studies, of the pharmacokinetic distribution of aluminum, as did an actual blood brain barrier scientist and yours truly. He also wrote a very good deconstruction of the claim that polysorbate 80 breaks […]
LikeLike
[…] several posts, the BBB scientist – an expert in the field of pharmacokinetics – also describes the […]
LikeLike